Introduction to periodontal regeneration
The ultimate goal of periodontal treatment is the regeneration of lost periodontal structures. Regeneration can be defined as the reproduction or reformation of organs or tissues that have been lost or injured as a result of a wound or infection. Periodontal regeneration results in functionally aligned periodontal ligament fibers between newly formed bone and the root surface. The periodontal regenerative procedure involves the creation of new alveolar bone, cementum, and periodontal ligament. The regeneration of periodontal tissues requires an appropriate biological environment which induces the differentiation of undifferentiated cells to make required structures. Various molecules such as growth factors and cytokines play a vital role in regeneration. A thorough knowledge of these molecules, as well as their functions, is required to understand the biological mechanisms involved in regeneration.
The events that take place during wound healing ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
General overview of wound healing
Wound healing has three principal phases: inflammatory, proliferative, and remodeling phase. The phases of wound healing are overlapping, but are described in a linear fashion for the purpose of clarity. Healing is also described as healing by primary intention or secondary intention. In healing by primary intention, the wound edges are apposed and there is minimal tissue loss. Healing by secondary intention is characterized by edges that are separated with a more extensive tissue loss. Healing by primary intention results in a small scar, whereas healing by secondary intention is followed by a large scar. In most of the periodontal surgical procedures, our main aim is to achieve primary healing. Let us now, discuss various phases of wound healing,
Inflammatory phase:
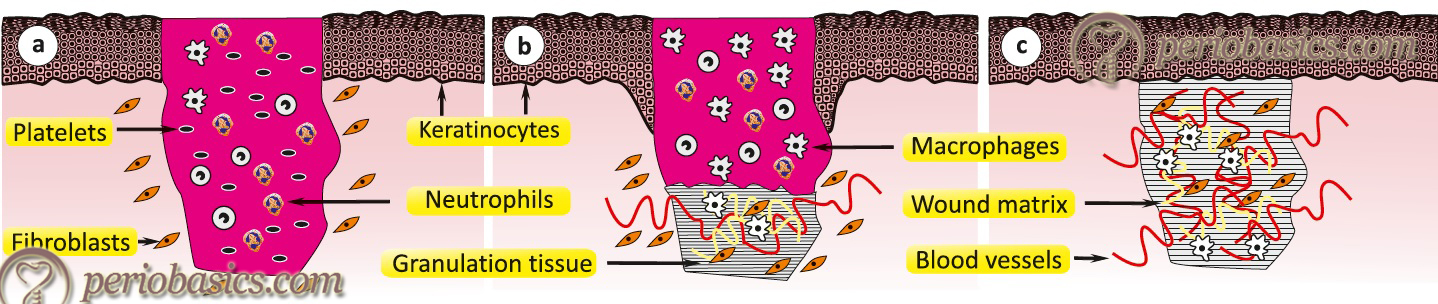
The inflammatory phase is characterized by hemostasis and inflammation. It begins at the time of injury and lasts for 24 to 48 hours. The healing process cannot proceed until hemostasis is accomplished. Collagen exposed during wound formation activates the clotting cascade (both the intrinsic and extrinsic pathways). The end product of the hemostatic process is clot formation which is primarily composed of fibrin mesh and aggregated platelets along with embedded blood cells. Fibrin mesh present in the clot acts as the wound matrix onto which fibroblasts and other cells migrate as the healing process proceeds. Platelets form the initial thrombus release growth factors that induce the chemotaxis and proliferation of neutrophils and macrophages, which co-operate to remove necrotic tissue, debris, and bacteria from the wound. Macrophages and neutrophils release ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
The degranulation products of platelets play a very important role during the initial inflammatory process. Alpha granules of platelets contain a variety of immunomodulatory and proteinaceous factors that are involved in both, the early and late phases of healing. These include factors like albumin, fibrinogen, fibronectin, IgG, and coagulation factors V and VIII, as well as platelet-derived growth factor (PDGF), transforming growth factor α and β (TGF-α and TGF-β), fibroblast growth factor-2 (FGF-2), platelet-derived epidermal growth factors (EGFs), and endothelial cell growth factor.
Monocytes in the nearby area are attracted to the area and transform into macrophages, usually around 48 to 96 hours after injury. Macrophages then become the prominent cells during this time period and release various growth factors and cytokines that change the relatively acellular wound into a highly cellular environment. Macrophages secrete important cytokines like IL-4, IL-5, IL-8, IL-12, IL-15 which play an important role in the activation of T-cell and B-cell mediated immune response.
Regulatory mechanisms ensure that growth factors and cytokines are present within the wound for sustained periods. For instance, lymphocytes are activated by macrophages to produce cytokines such as interferon-γ (INF-γ) that act back on macrophages and monocytes (in a paracrine manner) to release other cytokines such as tumor necrosis factor-α (TNF-α) and interleukin-1 (IL-1).
Proliferative phase:
During this phase, epithelialization, angiogenesis, granulation tissue formation and collagen deposition take place. Fibroblasts proliferate to become the dominant cell of the proliferative phase. They migrate into the wound site from the surrounding tissue, become activated, and begin synthesizing collagen. They proliferate in response to growth factors and cytokines that are released from macrophages, platelets or mesenchymal cells, or those that have been stored in the fibrin clot. In addition to chemotactically drawing fibroblasts into the wound, PDGF, FGF and EGF induce fibroblast activation and proliferation. Starting at day 3 or 4, collagen is deposited, net collagen deposition is positive until day 21. After this day, collagen deposition is in balance with collagen resorption and no further net collagen deposition occurs. Platelet-derived growth factor (PDGF) and epidermal ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Remodeling phase:
It begins at about 2 to 3 weeks and can last up to 2 years. Re-organization and remodeling of collagen (already deposited) take place during this period. Matrix metalloproteinases (MMPs) are intimately involved in the breakdown of collagen molecules. MMPs are zinc-dependent endopeptidases that cleave most macromolecules within the extracellular matrix. There are nine members of the MMP family, four of which are involved in wound repair 2. These are interstitial collagenases, stromelysins, gelatinases and membrane-type metalloproteinases. Osteoblasts-assisted bone formation and remodeling take place during this period.
Healing in the periodontium
Healing in the periodontium is in many ways similar to the healing in other parts of the body, but at the same time, it has some fundamental differences. Dentogingival junction is a unique structure associated with teeth. It is considered as the battlefield of bacterial and host immune response. So, during inflammation of the periodontium, its continuity is ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Research done on periodontal wound healing has provided us information regarding tissue response and how it can be modulated to achieve regeneration of lost periodontal structures. Guided tissue regeneration is an example of modulation of tissue response during healing.
With this basic information regarding wound healing process, let’s now discuss the cellular and molecular basis of periodontal regeneration.
Cellular and molecular basis of periodontal regeneration
To regenerate periodontal tissues, a combination of cellular and molecular activities are required. Cells such as epithelial cells, osteoblasts and fibroblasts play an important role in post-operative healing. As described in the previous section, the activated inflammatory cells produce various mediators which play specific roles during the healing process. Molecules such as growth factors, adhesion molecules and structural proteins play an equally important role. The signaling molecules that have been most intensively investigated in periodontal regeneration include bone morphogenetic proteins (BMPs, e.g. BMP-2, BMP-7, and BMP-12) 3-12, transforming growth factor (TGF)-β1 13, 14, platelet-derived growth factors (PDGFs, such as PDGF-BB) 15-18, insulin-like growth factor (IGF)-1 15, 19, 20, and basic fibroblast growth factor (b-FGF) 21-24. Let us discuss these components in detail,
Cellular components
Fibroblasts:
Fibroblasts synthesize the extracellular matrix and collagen, structural framework (stroma) for tissues, and play a critical role in wound healing. The main function of fibroblasts is to maintain the structural integrity of connective tissues by continuously secreting precursors of the extracellular matrix. Fibroblasts are derived from primitive mesenchyme, like all connective tissue cells. They play a vital role in periodontal regeneration as these are responsible for periodontal ligament formation.
Fibroblast activation:
Normal fibroblasts are embedded within the fibrillar extracellular matrix of the connective tissue and constitutively express vimentin and fibroblast-specific protein 1 (FSP1). The activated fibroblasts typically contain a large oval euchromatic nucleus with one or two nucleoli, rough endoplasmatic reticulum, and a prominent Golgi apparatus. Activation of fibroblasts takes place when tissue injury occurs. The injured epithelial cells and infiltrating mono-nuclear cells such as monocytes and macrophages release various factors like transforming growth factor-β (TGF-β), epidermal growth factor (EGF), platelet-derived growth factor (PDGF) and fibroblast growth factor 2 (FGF2), which also activate fibroblasts. In addition, fibroblasts are activated by direct cell-cell communication and contact with leukocytes through adhesion molecules such as intercellular adhesion molecule 1 (ICAM1) or vascular cell adhesion molecule 1 (VCAM1).
The activated fibroblasts secrete various mediators ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Osteoblasts:
Osteoblasts are specialized stromal cells that are exclusively responsible for the formation, deposition and mineralization of bone tissue. Bone formation is characterized by a sequence of events starting with the commitment of osteoprogenitor cells and their differentiation into pre-osteoblasts and then into mature osteoblasts, whose function is to synthesize the bone matrix that becomes progressively mineralized. It is a strictly regulated process.
Regulation of osteoblast activity:
Various growth factors, cytokines and molecules have been demonstrated to facilitate the proliferation and differentiation of osteoprogenitors to pre-osteoblastic and mature osteoblastic cells. Bone morphogenic protein (BMP) is a family of proteins that can act on early osteoprogenitors to instigate their differentiation to pre-osteoblastic cells 25. The most important regulatory system in bone formation and resorption is RANK (receptor activator of nuclear factor κB) / RANKL (RANK ligand) /OPG (osteoprotegerin) system. A detailed description of this regulatory system that controls bone remodeling, has been given in chapter 11 “Osteoimmunology in periodontal health and disease”.
Molecular components
Cytokines:
IL-1:
IL-1 is a representative proinflammatory cytokine that regulates many aspects of the immune and inflammatory responses. There are two IL-1 ligands with agonist activity, IL-1α and IL-1β, which are produced by various kinds of cells such as neutrophils, monocytes/macrophages and fibroblasts. Both IL-1α and IL-1β, bind to the same receptor and have similar, if not identical, biological properties. It has been shown that IL-1α and IL-1β expression strongly enhances during wound healing 26. IL-1α plays an important role during wound healing. It is known to be constitutively produced by epidermal keratinocytes under normal conditions, and injection of this cytokine enhances ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
TNF-α:
Tumor necrosis factor-α (TNF-α) is a pleiotropic cytokine produced by a variety of cell types including macrophages, T- cells, mast cells, and keratinocytes. In various concentrations it has inflammatory, cytolytic, mitogenic, antitumor, and possibly angiogenic or antiangiogenic effects; therefore it is likely to affect wound healing. There are two types of receptors for TNF-α encoded by distinct genes: TNF receptor with a molecular mass of 55 kDa (TNF-Rp55) and one with a molecular mass of 75 kDa (TNF-Rp75) 29. TNF-Rp55 mediates various activities of TNF-α, including cytotoxicity, fibroblast proliferation, and induction of superoxide dismutase whereas TNF-Rp75 mediates thymocyte and cytotoxic T-cell proliferation 30.
Interleukin 4 (IL-4):
IL-4 is secreted by Th2 lymphocytes, mast cells and macrophages, which stimulates a number of fibroblast activities such as migration, proliferation, and synthesis of the extracellular matrix 31. A late increase of IL-4 is found at the wound site is correlated with the decreased expression of several other cytokines 32, 33.
Interleukin 6 (IL-6):
It has mitogenic effects on epithelial cells and has a chemoattractive effect on neutrophils 34. IL-6 is also known as a potent stimulator of fibroblast proliferation 35 and it is important in inhibiting extracellular matrix breakdown during proliferation 36. It has been reported that a complete lack of IL-6 causes impaired wound healing 34. IL-6 performs an important function in acquired immunity by promoting specific differentiation of T- and B-cells. As for T-cells, IL-6 together with transforming growth factor (TGF)-β has been shown to be essential for Th17 differentiation from naïve CD4-positive T-cells, whereas, on the other hand IL-6 inhibits TGF-β-induced regulatory T-cell (Treg) differentiation.
Interleukin 8 (IL-8):
IL-8 is secreted by epithelial cells and macrophages. The expression of IL-8 is triggered by IL-1 and TNF-α 33 and correlates strongly with neutrophil infiltration at the wound site 37. IL-8 is a major chemoattractant for polymorphonuclear leukocytes. There are many receptors on the surface membrane capable of binding IL-8; the most frequently studied are the G protein-coupled serpentine receptors, CXCR1 and CXCR2. It is important to note that IL-8 can be secreted by any cells with toll-like receptors that are involved in the innate immune response.
Interleukin 10 (IL-10)
It is an anti-inflammatory cytokine involved in the limitation and termination of the inflammatory process. As a factor produced by T helper 2 (Th2) cells, IL-10 inhibits the production of cytokines by Th1 cells 38. IL-10 regulates growth and/or differentiation of immune cells, epithelial cells, and endothelial cells and inhibits infiltration of neutrophils as well as the expression of several cytokines 39. An increased ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Growth factors:
Over the last 20 years, there has been an immense increase in our knowledge about growth factors, cell adhesion molecules and cytokines, with a significant improvement in the understanding of the cellular and molecular biology of periodontal regeneration. Growth factors, cell adhesion molecules and cytokines play a vital role in healing and periodontal regeneration. The role of various growth factors during wound healing has been illustrated in following figure,
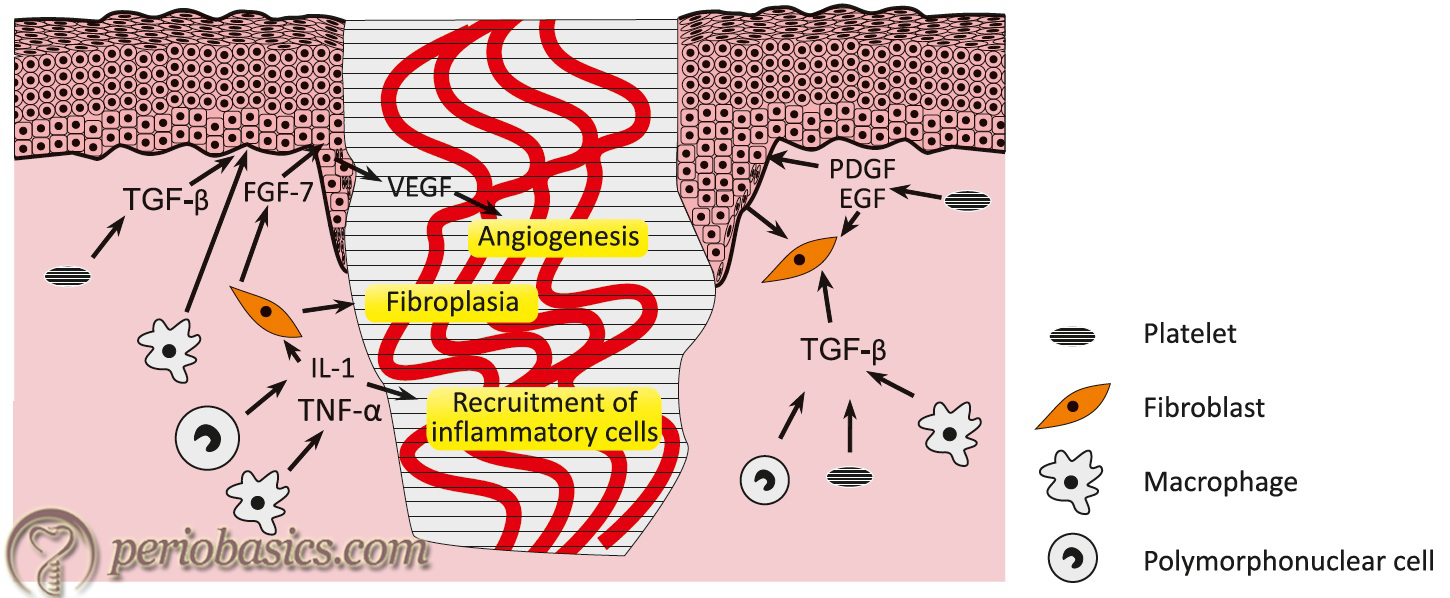
So, what are growth factors? Growth factors are naturally occurring substance capable of stimulating cellular growth, proliferation and cellular differentiation 43. Growth factors act as signaling molecules between cells. Following is a brief description of growth factors which have been our focus of research,
Platelet-derived growth factor:
Platelet-derived growth factor (PDGF) was purified from platelet extracts and is characterized as a mitogen for fibroblasts 44. It was originally purified from human platelets, but recently has been found to be produced by various other cells, for example, monocytes, megakaryocytes, vascular endothelium, smooth muscle cells, and transformed cells 45, 46. In humans, several dimeric isoforms are produced from four ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Platelet-derived growth factor (PDGF) in vitro stimulates DNA synthesis and chemotaxis of fibroblasts and smooth muscle cells and stimulates collagen, glycosaminoglycan, and collagenase production by fibroblasts. PDGF has been shown to potentiate regeneration of the periodontium in naturally occurring periodontitis in dogs 48 as well as in experimental periodontitis in monkeys 49.
| Various growth factors, their sources and their effects. | ||
|---|---|---|
| Growth factors | Source | Effect |
| Fibroblast growth factors 1, 2, 4 | Macrophages, endothelial cells | Fibroblast proliferation and angiogenesis. |
| Transforming growth factor-α | Macrophages, keratinocytes | Re-epithelialization. |
| Transforming growth factors β1, 2 | Platelets, macrophages | Fibroblast and macrophage chemotaxis. Extracellular matrix synthesis. Secretion of protease inhibitors. |
| Insulin-like growth factor | Plasma, platelets | Endothelial and fibroblast proliferation. |
| Platelet-derived growth factor (isoforms AA, AB and BB) | Platelets, macrophages, keratinocytes | Fibroblast and macrophage chemotaxis. Fibroblast proliferation. Matrix synthesis. |
| Epidermal growth factor | Platelets | Re-epithelialization. |
| Keratinocyte growth factor | Dermal fibroblasts | Keratinocyte proliferation. |
| Interleukin 1-α and 1-β | Neutrophils | Activate growth factor expression in macrophages, keratinocytes and fibroblasts |
| Tumor necrosis factor-α | Neutrophils | Activate growth factor expression in macrophages, keratinocytes and fibroblasts. |
Fibroblast growth factor-1 and -2:
Fibroblast growth factors (FGFs) play an important role, not only during normal development but also during wound healing. To date, twenty-two distinct FGFs have been discovered, numbered consecutively from 1 to 22. Out of these FGF-1 (Acidic FGF/ aFGF) and FGF-2 (Basic FGF/ bFGF) have been extensively studied for periodontal regeneration. Both FGF-1 and FGF-2 were initially isolated from bovine pituitary extracts based on their stimulation of [3H] thymidine incorporation in 3T3 fibroblasts 50, 51.
FGF-1 (Acidic FGF/ aFGF):
The human FGF-1 is a 155 amino acid protein. It is a well-known fibroblast activator, which acts through four specific cell surface receptors, among which, fibroblast growth factor receptor 4 (FGFR4) is highly specific. It is also known as the heparin-binding growth factor (HBGF)-1. aFGF is considered to function in several important physiological and pathological processes, such as embryonic development, morphogenesis, angiogenesis and wound healing.
FGF-2 (Basic FGF/ bFGF):
Human FGF-2 occurs in low molecular weight (LMW) and high molecular weight (HMW) isoforms. LMW FGF-2 is primarily cytoplasmic and functions in an autocrine manner, whereas HMW FGF-2s are nuclear and exert activities through an intracrine mechanism 52. FGF-2 contains four cysteine residues at amino acids 26, 70, 88 and 93. While the cysteines at ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Functions:
Major functions of FGFs include cell proliferation, cell migration, cell differentiation and angiogenesis. These are one of the main growth factors playing a vital role during wound healing.
Insulin-like growth factor:
The insulin-like growth factor family has three peptide hormones or growth factors: insulin, IGF-I, and IGF-II having approximately 50 percent of their amino acids in common. Insulin is synthesized in the beta cells of the pancreas as proinsulin, which is cleaved to form insulin and C-peptide. The IGFs, which are synthesized primarily by the liver, retain the C-peptide and have an extended carboxy terminus 53.
Insulin, IGF-I, and IGF-II bind specifically to two high-affinity membrane-associated receptors that are tyrosine kinases. These growth factors stimulate DNA synthesis and regulate development and differentiation in a large variety of cell types, thus playing a ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Bone morphogenetic proteins:
Bone morphogenetic proteins (BMPs) represent a unique set of differentiation factors that induce new bone formation. According to Bowers and Reddi (1992) 54 BMPs are proteins found in high amounts in bone tissues and are considered as responsible for inductive and regenerative abilities of demineralized bone grafts used in periodontal therapy. BMPs have a great potential in periodontal regeneration. A lot of research has already been done on their role during wound healing. A detailed description of BMPs is available in “Bone morphogenetic proteins in periodontal regeneration”.
Epidermal growth factor:
Epidermal growth factor is a small protein with only 53 amino acids. Cells that respond to EGF have receptors on the cell membrane that recognize the factor. The binding of the growth factor to the receptor initiates a cascade of molecular events involving the MAPK/ERK pathway that will eventually lead, along with other effects, to cell division. The cell membrane ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Application of growth factors in periodontal regeneration has been our focus in the recent past. A detailed discussion is required to thoroughly understand the structure and functions of these molecules because in future we are going to see a lot of research in this field. A detailed description of growth factors has been given in “Application of growth factors in periodontal regeneration”.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Adhesion molecules
Fibronectin:
Fibronectin (FN), a ubiquitous and abundant extracellular matrix protein, is secreted by cells as a soluble dimer and is subsequently assembled into insoluble multimeric fibrils at the cell surface. It is a glycoprotein found in a size of 220-250 kDa subunits linked by two disulfide bonds. This molecule is involved in adhesion and attachment of a variety of cells. In addition to its cell attachment functions, fibronectin is also involved in interactions with collagen, heparin and other cell surface glycosaminoglycans. It is a major component of extracellular matrix and is an important component of basement membrane. Besides acting as a barrier to macromolecules and cells, the basement membrane also provides a substratum for some cell types, supporting spreading, differentiation, and migration 58.
Fibronectin plays an important role during wound healing. It promotes the spreading of platelets at the site of injury, adhesion and migration of neutrophils, monocytes, fibroblasts, and endothelial cells into the wound region, and migration of epidermal cells through the granulation tissue. At the level of matrix synthesis, fibronectin appears to be involved, both in the organization of the granulation tissue and basement membrane. During tissue remodeling, it acts as a non-immune opsonin for phagocytosis of debris by fibroblasts, keratinocytes, and under some circumstances, macrophages. It also enhances the phagocytosis of immune-opsonized particles by monocytes 59.
Laminin:
Laminin is the most abundant glycoprotein in the basement membrane. It is both structurally and biologically active component of the basement membrane. Laminins are large (400-900 kDa) heterotrimeric molecules composed of one α, one β and one γ subunit in a cruciform or T-shaped appearance. To date, five α, three β and three γ chains have been characterized. They represent the products of distinct genes that evolved by duplication and recombination of ancestral α, β and γ genes, hence they share sequence similarity. Currently, the trimers are named ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Osteopontin:
Osteopontin is a secreted phosphoprotein containing the arginine-glycine-aspartate (RGD) tripeptide integrin-binding motif. It is also known as bone sialoprotein-1 (BSP-1 or BNSP). It is a highly negatively charged, extracellular matrix protein that lacks an extensive secondary structure. It is composed of about 300 amino acids and is expressed as a 33-kDa nascent protein; there are also functionally important cleavage sites. Osteopontin is biosynthesized by a variety of tissue types including fibroblast, preosteoblasts, osteoblasts, osteocytes, odontoblasts and some bone marrow cells, etc. Osteopontin has been implicated as an important factor in bone remodeling. It also binds to several integrin receptors, including α4β1, α9β1, and α9β4, expressed by leukocytes. It has chemotactic properties, which promote cell recruitment to the inflammatory sites.
Bone sialoprotein (BSP):
BSP is a highly glycosylated and sulfated phosphoprotein that is found almost exclusively in mineralized connective tissues. The polypeptide chain of BSP has a molecular weight of 35 kDa. BSP belongs to the SIBLING (Small Integrin-binding Ligand N-linked Glycoprotein) gene family 66 and displays several characteristics typical of these proteins. BSP is expressed by several cell types associated with mineralized tissues, but is expressed in abundance by osteoblasts. It binds to several distinct extracellular matrix constituents with diverse biological roles, including collagen 67, 68, factor H 69, matrix metalloproteinases 70, hydroxyapatite 71 as well as integrins present on numerous cell types 72-74.
Collagens:
Collagens are a group of closely related proteins that comprise the most abundant proteins found in mammals representing 25-35% of the total body protein 75. To date, at least 28 different types of collagen encoded by 45 genes have been identified 76, 77. A detailed description of collagen synthesis and structure has been given in, “Periodontium in health”. Collagen has many properties ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Cementum attachment protein:
Cementum attachment protein is a collagenous protein that is expressed in the matrix of tooth cementum. This protein binds with high affinity to the non-demineralized root surfaces, hydroxyapatite and fibronectin. It promotes the attachment of mesenchymal cells and may function in cementogenesis. This protein is capable of recruiting cementoblasts on the root surface during periodontal wound healing, thereby initiating new cementum formation. Integrin α5β1 is responsible for mediating the attachment of cementum attachment protein to the periodontal-derived cells, human gingival fibroblasts and human periodontal ligament fibroblasts.
Structural proteins
Structural proteins are the components of the basic framework of the connective tissue. Three major components of ground substance are,
Proteoglycans (glycosaminoglycans with proteins): chondroitin-4-sulfate, chondroitin-6-sulfate, dermatan sulfate, heparan sulfate, heparin.
Glycosaminoglycans (non-sulfated and sulfated): hyaluronic acid.
Glycoproteins: fibronectin, laminin, etc.
Proteoglycans are responsible for the highly viscous character of the ground substance. Proteoglycans consist of proteins (~5%) and polysaccharide chains (~95%), which are covalently linked to each other. The polysaccharide chains belong to one of the five types of glycosaminoglycans, which form the bulk of the polysaccharides in the ground substance. Hyaluronan (or hyaluronic acid) is the dominant glycosaminoglycan in the connective tissues which serves as a “backbone” for the assembly of other ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Intracellular signaling mechanism
All the growth factors, cytokines and other chemical mediators, act via a process known as receptor-mediated signal transduction. This process is activated by the binding of ligands such as growth factors, and cytokines to specific receptors. Before we discuss these intracellular signaling cascades, we should know about three general modes of signaling, named autocrine, paracrine and endocrine signaling.
Autocrine signaling:
In this signaling, cells respond to the signaling molecules that they themselves secrete. In this manner, an autocrine loop is established. Autocrine growth regulation can be seen in the proliferation of antigen-stimulated lymphocytes.
Paracrine signaling:
In this case, one cell type produces the ligand, which then acts on the adjacent target cells that express the appropriate receptor. The responding cells are in close proximity to the ligand-producing cell and are generally of a different type. Paracrine signaling is commonly seen in connective tissue repair during wound healing, in which a factor produced by one cell type (e.g., a macrophage) has a growth effect on the adjacent cells (e.g., a fibroblast).
Endocrine signaling:
In this type of signaling, one cell type produces the ligand, which then acts on distant target cells that express the appropriate receptor. Hormones synthesized by cells of endocrine organs act on target cells distant from their site of synthesis, being usually carried by the blood. Growth factors and cytokines also have systemic effects.
Receptors and signal transduction pathways
The binding of a ligand to its receptor triggers a series of events by which extracellular signals are transduced into the cell resulting in changes in the gene expression. Following signal transduction pathways have been described in case of growth factors and cytokines intracellular signaling,
Receptors with intrinsic tyrosine kinase activity:
This mechanism of activation is found in most of the growth factors such as EGF, TGF-α, HGF, PDGF, VEGF, FGF, c-KIT ligand, and insulin. Here, the receptor for the ligand has an extracellular ligand-binding domain, a transmembrane region, and a cytoplasmic tail that has intrinsic tyrosine kinase activity. When the ligand binds to the receptor, dimerization of the receptor, tyrosine phosphorylation, and ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Receptors without intrinsic tyrosine kinase activity that recruit kinases:
This signaling mechanism is found in many cytokines, such as IL-2, IL-3, and other interleukins; interferons α, β, and γ; erythropoietin; granulocyte colony-stimulating factor; growth hormones; and prolactin. These receptors transmit extracellular signals to the nucleus by activating members of the JAK (Janus kinase) family of proteins. After activation, JAK’s attach to and activate cytoplasmic transcription factors called STATs (signal transducers and activation of transcription), which directly shuttle into the nucleus and activate gene transcription.
G protein-coupled receptors:
Various ligands including chemokines, vasopressin, serotonin, histamine, epinephrine and norepinephrine, calcitonin, glucagon, parathyroid hormone, corticotropin, and rhodopsin signal through this mechanism. These receptors transmit signals into the cell through trimeric GTP-binding proteins (G proteins). They contain seven .……… Contents available in the book ………. Contents available in the book ………. Contents available in the book ………. Contents available in the book ………
Conclusion
The above description regarding the biology of periodontal regeneration is just an overview of the events that take place during periodontal wound healing and all the components that are required during periodontal regeneration. Presently, a lot of research work is going on at the molecular level to find out efficient and cost-effective methods to deliver biologically active molecules like growth factors at the site of healing to achieve regeneration of the lost tissue. With the background present discussion, we can now go ahead with a discussion of our present status of molecular research in periodontal regeneration. As already stated, growth factors play a very important role in periodontal regeneration. A detailed description of growth factors application and its limitations is available in “Application of growth factors in periodontal regeneration”.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.