Introduction
Presently, dental implants are widely used in dentistry. The replacement of lost teeth with dental implants is an effective and acceptable treatment modality. Social recognition and acceptance of implants in dentistry has shown a dramatic increase in recent years. Implant dentistry has evolved dramatically in the past few decades to reach the present status. In the following sections, we shall read about the historical aspect of dental implants.
Evidence of dental implant treatment in history
History of dental implant treatment is centuries-old. There is evidence available which proves that prehistoric people sought this technology 1, 2. The Maya civilization has been shown to have used the earliest known examples of endosseous implants (implants embedded into bone). Archaeologists in 1931 found a fragment of the female mandible of Maya origin, dating from about 600 AD. This female in her twenties had three tooth-shaped pieces of shell placed into the sockets of three missing lower incisor teeth. It was believed by the archaeologists that these shells were placed after death in a manner also observed in the ancient Egyptians. In 1970, the Brazilian ………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……..
The use of root form implants dates back thousands of years. Evidence have shown their use in various civilizations like Chinese, Egyptians and Incas 3.
The modern era of dental implants
Probably, the first description of the technique of modern dental implants was published by a French dentist, Maggiolo J. According to ME Ring (1995) 4, Maggiolo describes a method to implant 18-karat gold alloy, with three branches into the jawbone, and to install a porcelain crown as a superstructure in his book: “Le Manuel de l’Art du Dentiste” (1809). During mid-1800s Harris placed a porcelain implant in the jaw bone. The porcelain surface of the implant was made rough with the help of lead coating. During the later half of 1800s Berry constructed a root-form implant that was lead-free.
During the beginning of the 20th-century, research work on dental implants was initiated in different parts of the world. Various materials like aluminum, gold, silver, red copper and nickel were used to make dental implants 5. Scholl made a root-form, porcelain implant in 1905 that consisted of corrugated structure 6.
A latticed cage design of dental implant was given by Greenfield in 1909, which was made up of iridoplatinum 7. He also introduced trephine burs to place implants. In 1913, he placed a “24-gauge hollow latticed cylinder of iridioplatinum soldered with 24-karat gold” as an artificial root to “fit exactly the circular incision made for it in the jaw-bone of the patient. He was also the first one to report dental implant failure due to infection 4. In 1937, Stock at Harvard University introduced Vitallium®, a cobalt-chromium-molybdenum alloy which was used to make implants. A cylindrical endosseous implant that was threaded both internally and externally; it had a smooth gingival collar and a healing cap was patented by Dr. PB Adams in 1938. In 1940s post type endosseous implant was developed by Dr. Formiggini and Dr. Zepponi. During the same time period, Dr. Raphael Chercheve created burs that matched the diameter of spiral implants to ease the insertion of the implant for the best fit.
The fusion of titanium to bone was first reported in 1940 by Bothe et al. (1940) 8 which was the beginning of research work on titanium implants. Professor Per-Ingvar Brånemark, a Swedish orthopedic surgeon in 1952 started his extensive experimental study on the microscopic circulation of bone marrow ………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……..

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
By the mid 20th century, various procedures, techniques, and implant designs were introduced. Various thread designs were introduced during this time period. Leonard I Linkow of New York, in 1964 introduced self-tapping titanium implants. For cases with advanced bone loss, Linkow later created a blade implant that eventually became the most widely used implant design in the 1970s 10. In early 1980’s, Dr. Tatum introduced the omni R implant that consisted of horizontal fins made up of titanium alloy. During the same time period, Dr. Niznick introduced the Core-Vent implant. This implant was a hollow basket implant having a threaded piece in it, which helped to engage the implant to the bone. He also manufactured the Screw-Vent implant which had a hydroxyapatite coating on it.
The historical evolution of dental implants.
| Date | Innovation |
|---|---|
| 600 AD | The Mayan population used pieces of shells as implants to replace mandibular teeth. |
| 800 AD | Stone implants were prepared and placed in the mandible. |
| 1809 | J Maggiolo performed the first implant placement by inserting a gold implant tube into a fresh extraction site. |
| 1913 | E J Greenfield placed a hollow cylinder of Pt-Ir (24-gauge) soldered with 24-karat gold as an artificial root in the jaw-bone. |
| 1930s | Alvin and Moses Strock used orthopedic screw fixtures made of vitallium and placed in both humans and dogs to restore missing teeth. |
| 1938 | P B Adams placed a cylindrical endosseous implant. |
| 1940s | M Formiggini and F Zepponi developed a post-type endosseous implant. |
| 1940s | G Dahl developed a subperiosteal implant. |
| 1952 | Osseointegration discovered by Branermark. |
| 1960s | R Chercheve developed a double-helical spiral implant made of Co-Cr. |
| 1968 | L Linkow developed a thin and long blade implant to treat partial and total edentulism. |
| 1981 | Schroeder and Lendermann introduced titanium plasma spray. |
| 1983 | The first ceramic CAD/CAM solutions or prosthodontic restorations were developed. |
| 1988 | The All-on-4® treatment concept was introduced, which uses a reduced number of implants to treat full arches. |
| 2005 | Nobel Guide/Nobel Clinician introduced the first comprehensive concepts for 3D treatment planning. |
| 2005 | Immediate Function received clearance by the U.S. Food and Drug Administration (FDA). |
| 2011 | Thommen Medical introduced hydrophilic surfaces that speed early osseointegration. |
To summerize, four types of implant designs used were developed: intramucosal, subperiosteal, transosteal and blade implants. These designs are not used widely due to their high cost and unpredictability. Another problem is the un-predictable success rate with these systems. Some of these implants functioned reasonably well for years, some began to show signs of failure shortly after insertion 11.
Following is a brief description of these designs,
Intramucosal implants
Dahl in Germany (1943), developed button inserts, which are also known as intramucosal implants. These small metal buttons were incorporated into the tissue surface of a complete denture facing toward the patient’s tissue. Matching holes were surgically created in the patient’s denture-bearing soft tissue at diverging angles so when the denture was inserted; the buttons engaged and improved the retention of the denture. The problem with this design was that the patient had to wear the denture all the time because the surgically created hole in the mucosa would heal and denture insertion would be difficult or cause ulcerations in the tissue. Because of the drawbacks associated with this implant system, this system is rarely used today.
Sub-periosteal dental implants
Sub-periosteal implant placement was first described as a treatment for the atrophic mandible by Dahl in 1941. He placed a metal structure below the periosteum with vertical extensions protruding through the gingiva. These implants are used in very advanced alveolar bone resorption cases, where there may not be enough bone width or height for the more common and routinely placed type of implants: the root form implants. These implants were popularized by Goldberg and Gershkoff in 1946.
By definition, a sub-periosteal implant is a framework specifically fabricated to fit the supporting areas of the mandible or maxilla with permucosal extensions for support and attachment of a prosthesis. Initially, a mucoperiosteal flap was raised to take mandibular impression. CT scans were also used to allow CAD/CAM fabrication of the framework, negating the need for impressions. In this system, the framework usually rests on the mandible, with no penetration into the bone. The framework consists of ………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……..

Due to the high success rates of osseointegrated implants facilitated by the placement of autogenous grafts in atrophic mandibles, sub-periosteal implants are no longer used.
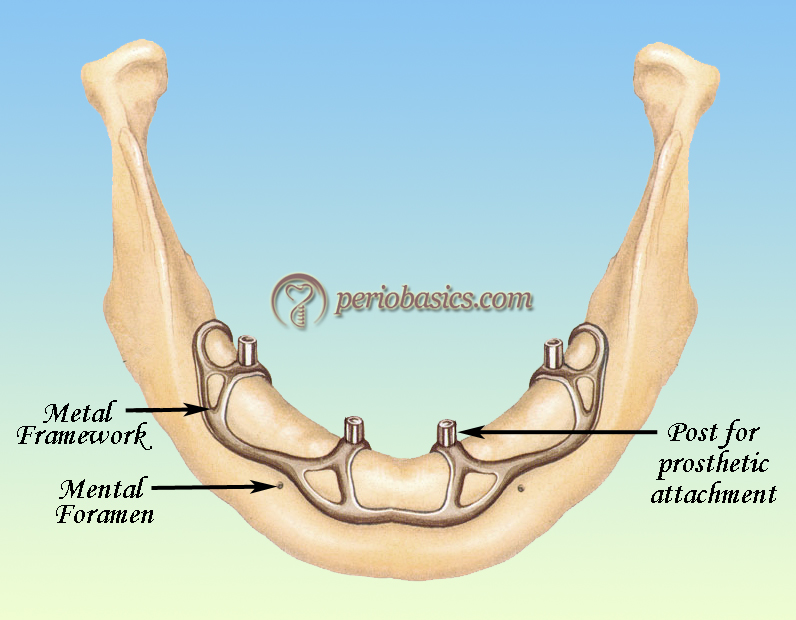
Trans-osteal implants
This system is used in mandible where the implants run throughout the body of the mandible and a metallic plate is utilized beneath the chin where these implants are attached. The posts projecting in the oral cavity are used to attach a removable prosthesis. There are specific contraindications for this form of implants, including patients having had radiation therapy to the jaws and prosthodontic or esthetic considerations. Because of the complexities involved in this system, it is no longer used these days.

Blade implants
The blade form implants were used in areas where the residual bone ridge of the jaw is either too thin (due to resorption) to place conventional root form Implants or certain vital anatomical structures prevent the placement of conventional implants. When the alveolar ridge is thin, it permits tricortical anchorage 12, i.e. the implant is stabilized by press-fit in both the internal and external bone cortex, as well as the deep cortex. This condition allows optimum stability for immediate loading of implants with a functional provisional prosthesis.
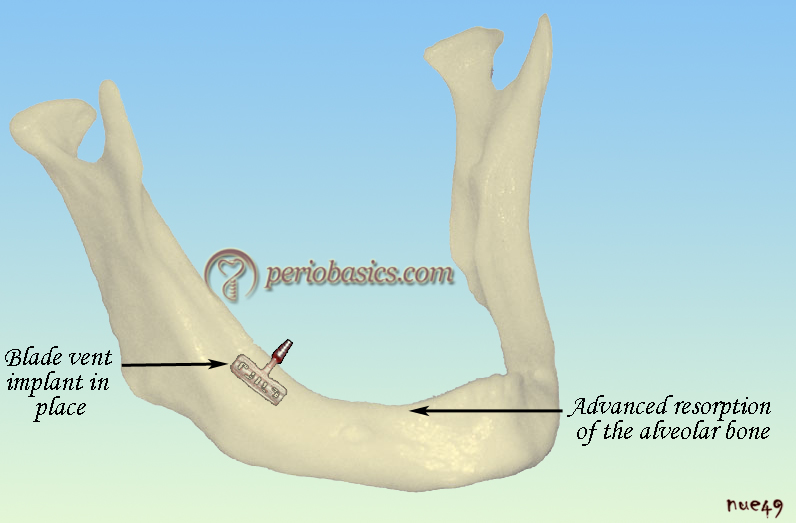
Here, the bone was split and the blade was inserted into the bone. As the bone formation takes place, these implants get firmly embedded into the bone. Presently these implants are rarely used because we have various bone augmentation procedures with the help of which we can put the endosseous root form implants successfully.
Other designs
Other less popular designs include one that utilized magnet implantation. Behrman and Egan in 1953 reported implanting magnets in patients’ jaws with an attractive magnet inside the patients’ complete denture. In 1967, Cowland and Lewis first described the vitreous carbon implant. Poor success rates have made this implant obsolete. Others have tried to use methyl methacrylate (acrylic resin) for implants, with little success.
Milestones in the development of modern implant dentistry
Concept of osseointegration
The most important milestone in the modern implant dentistry was the introduction of the concept of osseointegration. Professor Per-Ingvar Brånemark a Swedish orthopedic surgeon is considered as the father of modern dental implantology. He is one of the pioneer researcher who worked on osseointegration and started developing this method in the early 1960s. In 1982 in Toronto, Canada, he presented his research that began around 15 years earlier to explain the process of osseointegration, the biological ………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……..
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
During his research work on rabbits, Brånemark serendipitously discovered osseointegration of titanium optic chambers examined during vital microscopy. He found that titanium oculars placed into the lower leg bones of rabbits could not be removed from the bones after a period of healing 13. The Brånemark system is now marketed in the U.S. by Nobel Biocare. Another milestone was the introduction of self-tapping implants by Leonard I Linkow in 1964 10. He also introduced blade implants which were widely used.
In 1976 Dr. Andre Schroeder along with Straumann, studied titanium plasma-sprayed hollow endosseous implants and histologically demonstrated the in-growth of bone on the implant surface 14. In this way, the surface treatment of implants was introduced. Immediate implant placement after tooth extraction was reported by Professor Willi Schulte of the University of Tübingen in Germany. He used vitreous carbon implants. Their research work led to the development of Frialit-2 implant 15.
During 1980’s the Brånemark’s concept was widely explored and accepted. It led to further research on implant design and surface properties. Presently, we have numerous implant designs available with different surface properties providing us with one of the most promising treatment modality in dentistry.
Concept of fibrointegration
This concept was propagated by Weiss (1986) 16. According to him, there is a fibro-osseous ligament formed between the implant and the bone and this ligament can be considered equivalent to the periodontal ligament found around natural teeth. The collagen fibers are present at the bone-implant interface and have an osteogenic effect. He advocated the early loading of the implants.
Evolution of implant design
Before we go into the details of the evolution of implant design, let us first discuss the primary requirements of implant design. Requirements for an oral implant design included:
- Maximum surface area for attachment and primary stability;
- Anchoring effect with minor surface irregularities;
- Minimum bone loss during implant site preparation;
- Minimum implant body volume.
The preliminary designed implants had a hollow implant body as a basic design concept. Original endosseous implants were parallel in design. Early modifications in the hollow cylinder implants included transverse openings in the ………..Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……..
The screw-type implant concept was based on experience in the field of orthopedic surgery and other related research. The major advantage of this design was better biomechanical load distribution. These implants were designated as single tooth replacement implants. Other designs introduced included tapered implants and self-tapping implants. Self-tapping implants have been specifically designed for use in bones with poor quality (D3 and D4 bone). Presently, most implant companies offer tapered implants. The designs on the implant surface were also modified to improve the bone to implant contact and primary stability of the implant.

Surface modifications of dental implants
Modifying the surface of the implants is one of the most effective methods of improving the stability of the implant. Surface modifications of the implant have been shown to enhance the bone formation on its surface 17. Based on the scale of the surface features, the implant surface modification can be divided as macro-, micro- or nano-sized topographies 18, 19. The implant surface can be modified by ablative/ subtractive or additive procedures. Further information about these procedures is available in “Dental implant surface treatments”.
Conclusion
The dental implant treatment has become one of the most widely accepted and used treatment modality in dentistry. From the time of introduction of the concept of osseointegration by Professor Per-Ingvar Brånemark, till date, tremendous research work has taken place in the field of implant dentistry. Surgical techniques have been refined to help clinicians to achieve better primary stability of the implants. The present topic discussed briefly the development and evolution of implant dentistry to its present status. In the following chapter, we shall go into the detail of the biological aspect of dental implants.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.