Introduction
Various defense mechanisms active in the oral cavity include saliva, gingival sulcular/crevicular fluid, intact epithelial barrier (junctional epithelium), the presence of beneficial flora, migrating polymorphonuclear cells and other leukocytes, and local antibody production. The gingival crevicular fluid (GCF) and saliva play an important role in the defense mechanism of the oral cavity. Both GCF and saliva contain a variety of chemical mediators which serve various functions in the defense mechanism against infections. The composition of these fluids is different in inflammation as compared to periodontal health. This obser-vation has led to extensive research on these fluids to find out biochemical markers which can predict the presence of disease in the periodontal tissues. In the following discussion, we shall discuss in detail the formation, composition, and functions of GCF and saliva in oral health as well as the changes in their composition during periodontal diseases.
Gingival crevicular fluid (GCF)
The GCF has been extensively studied for more than 60 years. Waerhaug (1952) 1 while investigating the periodontal pocket of experimental dogs, administered India ink into their healthy gingival sulci. He observed that after one hour there was an increase in the transudation and emigration of leukocytes. The ink particles were almost completely eliminated from the gingival sulcus within next 48 hours. The results of this study suggested that fluid is formed in the gingival sulcus, which has a flushing action on the bacteria and debris present in the gingival sulcus. This was the initiation of research on GCF.
Later, a study by Brill and Krasse (1958) 2 highlighted that gingival sulcus was permeable to small molecular weight compounds. They administered fluorescein dye intravenously into the experimental animals to find out if it could penetrate the sulcular epithelium. The GCF from more than 90% of the animals was found to be positive for fluorescein dye, collected in strips of filter paper introduced into the sulcus as soon as one and a half minute after dye administration.
Subsequently, it was demonstrated that GCF is produced both in healthy as well as in diseased gingival sulcus 3, 4. The potential use of GCF as an indicator of periodontal diseases was then investigated by analyzing its composition in periodontal health and disease 5. The pioneer investigations on GCF enzymes were done by Bang and Cimasoni (1971, 1974) 6, 7. Subsequent ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Formation of GCF
Initially, it was proposed that GCF is formed due to inflammation in the connective tissue underlying the junctional and sulcular epithelium. Due to inflammation, there is an increase in the vascular permeability of the blood vessels resulting in extravascular fluid accumulation. This fluid was suggested to be the source of GCF. It was also demonstrated in earlier experiments that the permeability of the sulcular epithelium was different from that of other oral epithelia and the former was permeable to systemically administered fluorescein 4. It was shown that stimulation of the gingivae by tooth brushing or chewing 3, or intravenous injection of histamine or development of inflammation, markedly increased GCF flow 18. Brill et al. did extensive studies on GCF and concluded that it plays an important role in the transportation of antibacterial substances, either of host origin or those introduced into the circulation such as antibiotics and that the stimulation of gingiva was an important factor in the maintenance of gingival health 3-5, 19-23.
Another hypothesis regarding the formation of GCF was put forward by Pashley (1976) 24, who suggested that the un-stimulated GCF can be simply considered as an interstitial fluid which appears in the gingival crevice as a result of an osmotic gradient. According to this hypothesis, initial pre-inflammatory fluid in the gingival sulcus was transudate, which gets converted into inflammatory exudate on stimulation. This hypothesis was in agreement with the findings put forward by Alfano (1974) 25 who proposed that accumulation of bacterial plaque results in the accumulation of high molecular weight molecules at the basement membrane which creates an osmotic gradient. This osmotic gradient induces the flow of interstitial fluid from the connective tissue to the gingival sulcus. Further, recent research has shown that the GCF protein concentration in inflamed gingivae had a protein concentration similar to that of serum, suggesting it to be an inflammatory exudate 6, 21, 26. Hence, from the present evidence we can conclude that GCF in a healthy gingival sulcus is transudate, having a protein concentration similar to that of interstitial fluid.
Methods of GCF collection
There are many methods available for GCF collection. Each method has its own advantages and disadvantages. It must be noted that GCF collection should be completely atraumatic so that GCF fluid uncontaminated with blood can be collected. The method of GCF collection depends on the kind of investigation to be done on the GCF. Following is the description of commonly used methods for GCF collection,
Gingival washings method:
In this technique of GCF collection, the gingival crevice is perfused with a fixed volume of an isotonic solution such as Hank’s balanced salt solution. The technique was first explained by Oppenheim (1970) 27, where a customized acrylic stent is used to isolate the gingival sulcus from the rest of the oral cavity. Using a peristaltic pump, the gingival sulcus is irrigated with saline solution for 15 minutes and diluted GCF is collected 28. The collected fluid contains both cells and soluble constituents such as plasma proteins. The main advantage of this technique is that it can be used to harvest cells from the gingival crevice 29. This technique also has ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Skapski and Lehner (1976) 28 used a simpler technique to obtain crevicular washings from the gingival crevice. The process involved installation and re-aspiration of 10 μl of Hank’s balanced salt solution at the interdental papilla. This process was repeated 12 times to allow thorough mixing of the transport solution and GCF. The main advantage of this technique is that it can be used to obtain GCF fluid from a single site or multiple sites. The disadvantage of this technique is that it may not be possible to collect all crevicular fluid during aspiration and re-aspiration procedure. The precise composition and volume of GCF cannot be determined because it is not possible to determine the precise dilution factor.
Capillary tubing or micropipettes:
In this technique, the site from which GCF is to be collected is first dried and isolated. Then a capillary tube of known diameter is inserted into the crevice at its entrance. The crevicular fluid in the gingival sulcus migrates into the capillary tube by capillary action. Because the capillary tube of known diameter is used, the exact volume of GCF can be accurately determined 30. The main advantage of this technique is that undiluted sample of “native” GCF from isolated sites can be obtained and its volume can be accurately determined. However, the technique also has its own limitations. It is very difficult to obtain sufficient amounts of GCF, especially from non-inflamed sites. Sometimes, the collection time from an individual site may exceed 30 minutes and any trauma in the sulcus during this period may hamper the atraumatic collection of GCF. Sometimes it may be impossible to obtain an adequate sample of GCF from a healthy site. Another limitation of this technique is the collection of GCF sample from the capillary tube. Methods like, forcing out the solution with a jet of air and passing a larger fixed volume of a diluting solution through the capillary have been used to obtain GCF from capillary tubes for investigations 29.

Absorbent filter paper strips:
This is a simple and quick method of GCF collection, but variations in method of absorbent paper application, the timing of sample collection and estimation of the volume of GCF collected exist. There are two variants of this technique: intra-crevicular and extra-crevicular.

Intra-crevicular technique:
This is more commonly used technique where the absorbent paper is placed inside the gingival sulcus. This technique is further divided, depending on whether the strip is inserted just at the entrance of the crevice of periodontal pocket 5 or it is inserted till the base of the pocket or ‘until minimum resistance is encountered’ 22.
Extra-crevicular technique:
In this technique, the strip of absorbent paper is overlaid on the gingival crevice. By doing this, any trauma to the gingival crevice is avoided. However, by this method the amount of GCF collected is very small.
Estimation of GCF volume collected
The amount of GCF collected in absorbent paper has been estimated by various methods. The earlier methods utilized the linear measurement of the distance to which the fluid had migrated on the absorbent strip. To improve the accuracy of estimation, area of the absorbent paper wetted by GCF was measured. Staining the absorbent strips with ninhydrin stain which produces a purple color in the area where GCF had accumulated further improved the estimation of GCF fluid 31. However, the staining technique had some major dis-advantages such as the technique was not easily suitable for chairside usage, delay in measurement caused variations in estimation due to evaporation of the fluid and staining of proteins in GCF prevented further laboratory investigations of GCF components.

The introduction of Periotron® allowed accurate determination of GCF volume and facilitated further laboratory investigations on GCF components. This instrument is based on the principle of capacitance. When a dry absorbent strip is placed between two metal ‘jaws’ of the instrument (which act as the plates of an electrical condenser), the capacitance is translated via the electrical circuitry and registers ‘zero’ on the digital readout. After absorbing GCF from the gingival crevice, the absorbent strip is again placed on the instrument. Due to the wet area, the capacitance is increased which is proportional to the amount of fluid absorbed. The readings provide ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
| Periotron® reading | Level of gingival inflammation | Gingival index |
|---|---|---|
| 0-20 | Healthy | 0 |
| 21-40 | Mild | 1 |
| 41-80 | Moderate | 2 |
| 81-200 | Severe | 3 |
Problems associated with GCF collection and data interpretation
GCF contamination:
The three major sources of GCF contamination are blood, saliva, and plaque. Any injury to the sulcular epithelium may result in bleeding, which contaminates the GCF sample. Any sample with visible blood contamination should be discarded. Another major source of GCF contamination is plaque. Studies have shown that plaque significantly affects the GCF volume estimation 33, 34. To avoid contamination with plaque, it should be made sure that the site is completely free of plaque. Another contaminant during GCF sampling is saliva. If the site from where GCF sample has to be taken is isolated adequately, there are minimum chances of contamination by saliva. The presence of α-amylase in the sample has been used to confirm, or refute the saliva contamination of the GCF sample 35.
Determination of GCF volume:
During the determination of GCF volume, two major problems faced are evaporation of the fluid from GCF sample and errors in the estimation of smaller GCF volume (0.2 μL or less). Although introduction of Periotron® has significantly reduced the errors which may happen due to evaporation, these errors are significant when collected volume of GCF is low.
Sampling time:
Initially, 5 seconds was the time recommended for GCF collection with absorbent strips analyzed by Periotron®. But, the volume of GCF collected during this time was insufficient for laboratory analysis. Therefore, alternative techniques with more sample collection time were recommended. The techniques included placing a single absorbent strip for a longer duration of time or use of a sequence of repeated strips, with possible recovery periods in between. These techniques aimed at the collection of adequate GCF sample for laboratory analysis. The problem associated with prolonged collection time is the change in the nature of GCF with duration of collection time. The protein concentration of the GCF sample collected initially resembles that of interstitial fluid whereas prolonged samples have protein concentration approaching to that of serum 36.
Recovery of GCF from absorbent strips:
Another problem associated with GCF analysis is its recovery from absorbent strips. The GCF is primarily collected for biochemical analysis of its components. Recovery of proteins from GCF depends on the type of absorbent strip used, binding of GCF proteins to filter paper and concentration of the original proteins in the sample. It has been shown that using a centrifugal elution technique, the GCF protein recovery was close to 100% 37.
Composition of GCF
The composition of GCF may be broadly regarded as the result of interplay between the bacterial biofilm adherent to the tooth surfaces and the cells of the periodontal tissues. The cellular components of GCF are 70-80% granulocytes, 10-20% monocytes/macrophages, 5% mast cells and 5% T-lymphocytes. Many biochemical mediators ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
As already stated, GCF is either a serum transudate in a healthy, almost inflammation-free gingiva or more commonly an inflammatory exudate in the inflamed gingiva. The inflammatory cells are commonly seen in GCF fluid, particularly polymorphonuclear granulocytes (PMN), which are attracted by chemotactic gradients of bacterial or host origin. GCF is rich in bacterial products like endotoxins and host-derived molecules from the blood. Molecules like leukotriene B4 (LTB4), PAF, thromboxane B2, elastase and collagenase identified in GCF are derived from neutrophils 39. Monocytes/macrophages secrete mediators of inflammation such as PGE2, IL-1, IL-6, IL-8, and TNF.

GCF analysis
The GCF has been extensively subjected to protein analysis to understand its composition during inflammation and its potential use as a biomarker for disease activity. A site-specific analysis of the proteins can be done to analyze a particular component of GCF. At one point in time, a single analyte is usually investigated due to the small volume of GCF collected. Various techniques employed for protein analysis include,
- Western blot.
- ELISA.
- Multiplex protein analysis.
Western blot:
This test uses gel electrophoresis to separate denatured proteins by mass. After electrophoresis, proteins are transferred onto the membrane where they are made to react with specific antibodies. Subsequently, a secondary antibody which is covalently attached to an easily assayed enzyme or radiolabel binds to the primary antibody. After the antigen-antibody reaction is over, either autoradiography or chemiluminescence are used to detect radiolabeled antibodies or enzyme-labeled antibodies, respectively. The film with the bound proteins can be kept for a long time and can be scanned at any time to quantify the protein levels.
ELISA:
ELISA or the enzyme-linked immunosorbent assay is a plate-based assay, designed for detecting and quantifying substances such as peptides, proteins, antibodies, and hormones. It is based on the principle of using an enzyme-linked to an antibody or antigen as a marker for the detection of a specific protein, especially an antigen or antibody. The quantitative reading is usually based on detection of the intensity of transmitted light by spectrophotometry at a specific wavelength. More details regarding this test are available in “Advanced diagnostic techniques in periodontics”.
Multiplex protein analysis:
A multiplex assay is a type of assay that simultaneously measures multiple analytes (dozens or more) in a single run/cycle of the assay. This assay is used to detect multiple biomolecules of a given class (e.g., m-RNA or proteins) in a biological sample of GCF.
Potential of GCF as a source of biomarkers
As already stated, the difference in concentration of various components of GCF in healthy and diseased periodontium has led to an extensive research on its composition. The major driving force for GCF research is focused towards establishing a “diagnostic marker” for diseased periodontium. In a review, the potential diagnostic markers for periodontitis were highlighted, including, alkaline phosphatase, β-glucuronidase, cathepsin B, collagenase-2 (MMP- 8), gelatinase (MMP-9), dipeptidyl peptidase (DPP) II and III, and elastase 40. The components of GCF which can be used as potential biomarkers for periodontal disease can be discussed under three headings,
- Host-derived enzymes and their inhibitors.
- Tissue breakdown products.
- Inflammatory mediators and host response modifiers.
Following is the description of various components of GCF which have a potential use as a biomarker,
Host-derived enzymes and their inhibitors:
Alkaline phosphatase (ALP):
ALP is a host-derived enzyme that hydrolysis organic phosphate ester linkages which play a key role in bone homeostasis. This enzyme is released from PMNs during inflammation, osteoblasts during bone formation and periodontal ligament fibroblasts during periodontal regeneration 41, 42. The main source of ALP in GCF is ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Aspartate aminotransferase (AST):
This is an enzyme which is released into the extracellular environment after cell death. Elevated levels of AST in GCF have been reported at sites with active periodontitis as compared to healthy sites 45. Attachment loss and inflammation result in increased levels of AST in GCF 46. A chairside diagnostic system, Periogard TM (periodontal tissue monitor), has been developed which detects levels of AST in GCF 46, 47 (discussed in detail in “Advanced diagnostic techniques in periodontics”).
β-glucuronidase:
β-glucuronidase is a PMN derived lysosomal acid hydrolase, which is stored in primary azurophilic granules 48. It is involved in the destruction of noncollagenous components of the extracellular matrix and is considered as an indicator or predictor of periodontal disease activity 49. Levels of β- glucuronidase in GCF have been found to be significantly higher in active sites as compared to inactive sites 17. In poorly controlled diabetic patients, the levels of β-glucuronidase, collagenase and elastase have been detected significantly higher as compared to well-controlled diabetic patients 50, indicating their correlation with periodontitis in poorly controlled diabetic patients. This enzyme has also been shown to be a good predictor for future periodontal breakdown 51, 52.
Cathepsin B:
In GCF, macrophages are the main producers of cathepsin B 53. This enzyme has an important physiological role in the intracellular degradation and turnover of proteins in the lysosomal system. This enzyme can be used as a good indicator of periodontal disease activity because it degrades extracellular matrix proteins such as collagens, it modulates various inflammatory mediators and is released extra-cellularly by inflammatory stimulation. GCF concentrations of cathepsin B were found to be elevated in patients with periodontal disease, but lower in patients with gingivitis 54. A significant correlation has been demonstrated between GCF levels of cathepsin B and clinical parameters before and after periodontal treatment, suggesting that this enzyme can be used to assess treatment outcomes 40.
Cathepsin D:
Cathepsin D is a carboxy endopeptidase which is present in high concentration in the inflamed tissues. This enzyme is considered to be involved in the breakdown of the extracellular matrix. During active periodontal destruction, levels of cathepsin D in GCF have been shown to be 10 times higher as compared to GCF from healthy sulcus 55.
Elastase:
It is a potent proteolytic enzyme found in lysosomal granules that are released into the gingival crevice as a result of host-microbial interactions. It plays a role in the degradation of a wide range of extracellular matrix proteins, including fibronectin, laminin, proteoglycans, collagens, and elastin. It has been shown that levels of elastase in GCF during experimental gingivitis are elevated, which are reduced when plaque removal is reinstituted 56. Also, elevated levels of this enzyme in GCF have been reported in periodontitis 57.
Elastase inhibitors:
The activity of proteases in tissue is restricted by various naturally occurring protease inhibitors produced locally or derived from plasma. In plasma, primarily α2-macroglobulin and α1-antitrypsin are responsible for more than 90% of anti-protease activity. The α2-macroglobulin inhibits all the three neutral proteinases derived from PMNs by……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Matrix metalloproteinases (MMPs):
These are a family of proteolytic enzymes involved in the degradation of a variety of extracellular matrix macro-molecules such as collagens (interstitial and basement membrane), fibronectin, laminin and proteoglycan core protein. These enzymes are secreted in the latent state into the extracellular environment where they are activated. A detailed description of MMPs is available in “Matrix metalloproteinases and their role in periodontal diseases”.
The neutrophils are the major cells responsible for MMP release at the infected sites, specifically MMP-8 (collagenase-2) and MMP-9 (gelatinase-B). These are the main collagen-degrading enzymes in GCF and saliva 59, 60. There is a large body of evidence which suggests that the levels of MMPs are elevated during inflammation and active periodontal destruction 61, 62. Further, periodontal treatment has been shown to result in decreased GCF levels of MMPs 63. Studies have shown that levels of MMP-8 64, 65, MMP-3 66 and MMP-13 67, 68 are associated with the periodontal disease progression. One study demonstrated elevated levels of MMP-9 and MMP-2 gelatinases in subjects with periodontitis than the healthy subjects 60. The tissue inhibitors of matrix metalloproteinases (TIMPs) have a protective role for connective tissue. It has been suggested that tissue degradation is induced by an imbalance between MMPs and TIMPs 69.
Myeloperoxidase (MPO):
This enzyme is a major constituent of the azurophilic granules of PMNs. It is involved in the oxidation of chloride ions to the strong oxidant HOCl, which is the most bactericidal oxidant produced by the neutrophils 70. The azurophilic granular products are released into the phagosomes, so the extracellular release of this enzyme is mainly following neutrophil lysis 71. Because MPO is a major indicator of PMN infiltration, the GCF myeloperoxidase has been suggested as a good indicator of periodontal disease activity 72, 73. It has been demonstrated that in aggressive periodontitis, elevated levels of MPO are associated with amplified PMN activity as compared to chronic periodontitis where levels of GCF myeloperoxidase have been found to be comparatively less 69. Another study demonstrated that in patients with progressive chronic periodontitis, GCF myeloperoxidase levels are elevated, which are reduced in response to periodontal treatment 65.
Arylsulfatase:
This enzyme mediates the hydrolysis of sulfates and the metabolism of mucopolysaccharides. It is stored in lysosomes and is identified in higher concentration in the inflamed tissue. In one study, it was demonstrated that β-glucuronidase and arylsulfatase levels in the GCF were elevated in inflamed sites as compared to healthy, non-inflamed sites and that these levels decreased following periodontal treatment 74.
Tissue breakdown products:
Glycosaminoglycans (GAGs):
The levels of GAGs in GCF are good indicators of underlying tissue turnover. One study investigated sulfated glycosaminoglycans (hyaluronan and chondroitin-4-sulfate) in the crevicular fluid of patients with chronic adult periodontitis. The results of the study showed that significantly higher levels of chondroitin-4-sulfate were detected at diseased sites prior to the treatment which correlated with increased pocket depth or attachment levels 75. A study was ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Hydroxyproline:
Hydroxyproline is a major product of collagen breakdown. In one study, hydroxyproline and pyridinoline cross-linked carboxy-terminal telopeptide fragments of collagen Type I, which are connective tissue catabolism products, were studied. The results of the study showed that they may serve as direct measures of connective tissue catabolism for both soft and hard tissues 78. Akalin et al. (1993) 79 investigated hydroxyproline and total protein levels in gingiva and GCF in patients with juvenile, rapidly progressive, and adult periodontitis. Their results showed that the levels of both total proteins and hydroxyproline were raised in patients in the diseased groups as compared to a healthy control group. However, the authors did not support the concept that hydroxyproline and total protein levels in gingiva and GCF can be used as a suitable and a reliable criterion in the determination of disease activity.
Fibronectin fragments:
Fibronectin is a major component of the extracellular matrix (ECM). Its primary role is in cell adhesion and proliferation, which explains its potential use in regenerative strategies. The fibronectin fragments are produced by the degradation of the ECM. Estimation of their levels in GCF can be used as a marker to determine periodontal disease activity. Research has revealed that fibronectin is invariably found in a degraded form in the GCF 80, 81. However, its potential use as a biomarker is still to be established.
Bone specific matrix proteins:
The periodontal tissue destruction via osteoclastic action results in the sequestration of bone-specific matrix proteins like,
- Telopeptides of collagen Type I 82,
- Osteocalcin 83,
- Osteonectin 84,
- Osteopontin 85, and
- Bone phosphoprotein 86.
These products can be detected in the GCF and the levels of these markers in GCF have been associated with the progression of periodontal destruction. Following is the description of these proteins,
Osteonectin:
Osteonectin is a bone-specific protein that binds selectively to both hydroxyapatite and collagen. It is the most abundant glycoprotein secreted by human osteoblasts in the developing bone and odontoblasts in the developing teeth. Osteonectin levels in GCF have been investigated as a biomarker for the periodontal disease progression 86. However, more evidence is required to establish its use as a marker for bone-specific degradation product during the periodontal breakdown.
Osteocalcin:
Osteocalcin is a small (5.4 kDa), calcium-binding protein of bone, which accounts for 10-20% of the non-collagenous proteins in the bone matrix. Structurally, it has three residues of a calcium-binding amino acid, gamma-carboxyglutamic acid (Gla) which allows specific conformational changes, enabling its binding to ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Collagen Type I peptides:
The breakdown products of Type I bone collagen are the reflection of the osteoclastic activity of the bone 91, 92. Collagen Type I carboxy-terminal propeptide and collagen Type III amino-terminal propeptide are the product of the degradation of mature bone collagen Type I and are released during bone resorption. During periodontal bone resorption, these peptides are eliminated through the gingival pocket where they can be measured in the GCF. One study demonstrated that these collagen breakdown markers were identifiable in GCF of patients with periodontitis, but not in healthy subjects. Also, GCF levels of these collagens are increased after nonsurgical periodontal treatment, and return to baseline levels after a few days 80, 81.
Osteopontin (OPN):
Osteopontin is a phosphorylated, sialic acid-rich, non-collage-nous bone matrix protein. Structurally, it is composed of a single chain polypeptide composed of about 300 amino acids. OPN is produced by both osteoblasts and osteoclasts and its primary functions are bone mineralization, regulation of immune cell function and inhibition of calcification. OPN levels increase in active sites of bone metabolism. Studies have demonstrated that OPN level in GCF increases with the progression of periodontal disease 85, 93.
Laminin:
It is an integral component of the basement membrane. In response to the chemotactic signal, PMNs migrate into the connective tissue and move towards the inflammatory lesion. Some of these invade the gingival crevice. The destruction of the basement membrane is primarily done by activated PMNs 94. It has been demonstrated that the GCF levels of laminin are elevated in patients with periodontitis, which has been correlated to the presence of hyperactive neutrophils during the transmigration process through the endothelium/ epithelium 95.
Calprotectin:
Calprotectin is a 36.5 kDa calcium and zinc-binding protein consisting of one light (8 kDa, MRP8) and one heavy (14 kDa, MRP14) subunit. It belongs to the S100 protein family 96. This protein is expressed in the cytosol of neutrophils, monocytes, activated macrophages, and keratinocytes. It is released during activation or death of these cells. Studies have demonstrated that calprotectin is an inflammatory marker of periodontal disease 97-100. It was demonstrated in one study that ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Pyridinoline cross-links (ICTP):
Pyridinoline cross-linked carboxyterminal telopeptide of collagen Type I (ICTP) is derived from the carboxyterminal telopeptide regions of collagen Type I cross-linked via pyridinoline or deoxypyridinoline 106. It has emerged as a very promising biomarker of bone resorption in an array of osteolytic diseases. Many investigations have demonstrated a relationship between ICTP and high/low bone turnover diseases such as post-menopausal osteoporosis 107, 108. The GCF levels of ICTP have also been associated with bone and attachment loss in periodontitis 82, 109, 110. In a ligature-induced experimental periodontitis study on dogs, the GCF levels of pyridinoline cross-links (C-telopeptide and deoxypyridinoline) significantly increased during the development of attachment loss and osteoclastic bone resorption 77. Research has also shown elevated levels of ICTP in periodontitis cases exhibiting high levels of putative periodontal pathogens, including Tannerella forsythia, Porphyromonas gingivalis, Fusobacterium nucleatum subspecies, and Treponema denticola 112.
Inflammatory mediators and host response modifiers:
Cytokines:
Various cytokines are released during periodontal inflammation which can be detected in GCF and hence can be used as biomarkers for periodontal disease progression. These cytokines include Prostaglandin E2, Thromboxane B, IL-1, -6 and -8, tumor necrosis factor, etc. Pro-inflammatory cytokines, in particular, IL-1 β may play an integral role in the etiology of periodontal diseases. One study demonstrated that with an increase in the gingival index and probing, there was a corresponding increase in IL-1β in both the gingival tissue and GCF 113. On the other hand, reduction in IL-1 concentrations are associated with successful treatment 114. It has been shown that increasing severity of periodontitis is associated with increased concentrations of IL-1 and decreased concentrations of IL-1ra 115.
IL-2 has primarily been associated as an autocrine factor for T-cells, although some data indicate the ability of this factor to stimulate B-lymphocytes. Some reports have provided evidence for the presence of IL-2 in GCF, indicating activation of T-lymphocytes in the periodontium 116.
IL-8 primarily affects neutrophils and its levels in GCF is good indicator of progression of periodontal disease 117, 118. Some studies have found that the total amount of IL-8 is higher in diseased as compared to healthy sites 119 whereas others have reported an inverse relationship between PMN recruitment, responsible for ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Interferon-α (IFN-α):
IFN-α forms are produced by monocytes/macrophages, lymphoblastoid cells, fibroblasts, and a number of different cell types. Since IFN-α is produced by Th 1 cells, its levels in GCF are indicative of a cell-mediated immune response. Reduced levels of IFN-α at a site may signify a lowered cell-mediated immune response. In a study, it was concluded that the combination of decreased IL-8 and decreased IFN-α concentrations in GCF at diseased sites may reflect the reduced anti-bacterial host defense activity at that site 119.
Leukotriene B4 (LTB4):
It is an arachidonic acid metabolite produced via 5-lipoxygenase enzymatic pathway. It is produced from a variety of cells, including neutrophils, macrophages, and eosinophils. It possesses a variety of biological actions during the inflammatory response. It is a very potent activator of PMNs initiating their chemotaxis, aggregation, and adhesion to the endothelial cells. It also causes the lysosomal enzyme release and superoxide production in neutrophils. Other functions of LTB4 include increased vascular permeability, thereby contributing to an increased inflammatory response. It can modulate lymphocyte functions by stimulating INF-γ and IL-2 production from T-cells, and increasing IL-1 synthesis by monocytes. The GCF concentration of LTB4 has been found to be increased in areas of inflammation, suggesting its role in regulating the inflammatory response at sites with active periodontal destruction 126.
Prostaglandin E2 (PGE2):
PGE2 is known to have an activity on fibroblasts and osteoclasts to induce the synthesis of MMPs, IL-1β, and other cytokines. Levels of PGE2 in GCF have been detected to be increased in gingival tissue proportional to the severity of periodontal disease 127. Another study done on diabetic patients showed that there were significantly higher levels of IL-1β and PGE2 when compared with non-diabetic controls with similar periodontal status. Also, the levels of IL-1β and PGE2 increased in diabetics as the severity of periodontal disease increased 128.
RANTES:
RANTES (regulated on activation, normal T-cells expressed and secreted) is a chemokine that selectively attracts and activates macrophages and lymphocytes. In gingival inflammation, this chemokine is involved in the recruitment and activation of leukocytes. It has been demonstrated that RANTES is present in GCF of patients with periodontitis and is undetectable in healthy subjects 129. Another study reported that monocyte chemoattractant protein-1 (MCP-1) and RANTES could play key roles in both activation and recruitment of inflammatory and immune cells in the periodontal environment of patients with generalized Grade C (aggressive) periodontitis 130.
Acute-phase proteins:
Major acute phase proteins investigated in GCF in periodontitis include the C-reactive protein (CRP), protease inhibitors α2-macroglobulin (α2-M) and α1-antitrypsin (α1-AT) and the iron-binding proteins transferrin (TF) and lactoferrin (LF).
C-reactive protein (CRP):
C-reactive protein (CRP) is considered to be an important acute phase-sensitive marker of infectious burden and/or inflammation. It is considered as the best indicator of an individual’s systemic inflammatory status 131. It was first reported by Tillett and Francis in 1930 132 and was named so because it was discovered as a substance in the serum of patients with acute inflammation that reacted with the C-(capsular) polysaccharide of Pneumococcus. In a healthy individual, the CRP is a trace protein present in ng/ml quantities in the serum, but following tissue injury, its concentration may increase dramatically to hundreds of μg/ml within 72 hrs. The CRP binds to polysaccharides such as phosphocholine moieties present on the cell surface of many pathogenic microbes in the presence of calcium ions and activates the classical complement pathway, thereby opsonising the pathogen.
CRP is an acute-phase reactant produced ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Protease inhibitors α2-macroglobulin (α2-M) and α1-antitrypsin (α1-AT):
As already stated, one of the primary regulators of both endogenous and exogenous proteases, having an important role in the regulation of proteolytic activity at inflammatory sites is broad-spectrum protease inhibitor, α2-M. In a study done on smokers with severe periodontitis, significantly lower concentrations and total amounts of GCF α2-M and α1-AT were found as compared to healthy patients. The findings suggested that decreased concentration of these proteins may result in increased tissue damage due to increased activity of elastase and collagenase 136.
Transferrin (TF):
TF is a serum derived iron binding glycoprotein which binds more than 90% of iron in plasma. It functions in the absorption, transport, and exchange of iron in tissues. TF has been shown to have antibacterial activity. In GCF, significantly increased levels of TF have been found during diseased state 137.
Lactoferrin (LF):
Lactoferrin is an iron-binding protein present specifically and, in abundance, in the secondary granules of PMNs. Human LF is an 80 kDa glycoprotein with an 8.7 isoelectric point. LF is an important antimicrobial protein and it exerts its antimicrobial action due to its high affinity for iron. It acts on bacteria by causing iron depletion and thus resulting in a reduction in the bacterial cell division rate, glucose metabolism, and macromolecular synthesis. Also, LF facilitates phagocytosis of plaque bacteria by reducing their hydrophobicity and preventing their adherence. Since LF is the main component of neutrophil granules, its presence in saliva and GCF may be a good indicator of host-bacterial interactions. The normal levels of LF in the crevicular fluid are around 1.23 mg/l. It has been demonstrated that the GCF lactoferrin levels in chronic periodontitis patients are higher than in periodontally healthy individuals 138. Also, higher levels of LF have been found in the GCF of gingivitis and periodontitis patients as compared to healthy subjects 139. One study demonstrated a significant reduction in LF levels in the crevicular fluid following the surgical periodontal treatment 140.
Antibodies:
During periodontal inflammation in the established stages of periodontitis, immunoglobulins from the dense plasma cell infiltrate get access into the GCF. The antibodies formed against periodontopathogenic bacteria have been identified in GCF of periodontitis patients and attempts have been made to find an association between the presence of antibodies in GCF and periodontitis.
IgG:
The IgG antibodies play an important role in the prevention of periodontal destruction in patients with Grade C (aggressive) and Grade A/B (chronic) periodontitis. Complement activation is possibly the most important biological function of IgG. The complement cascade is initiated by binding of C1 to sites on the Fc portion ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
IgA:
Serum IgA is monomeric, but IgA found in secretions is a dimer having a J chain. It does not normally fix complement and has been demonstrated to be a potent inhibitor of complement activation by IgG 141. It has been isolated in GCF and is proposed to have anti-inflammatory effects. It hinders the attachment of pathogens to the tooth surface and thus prevents bacterial adherence and proliferation in the subgingival environment. The GCF levels of IgA have been found to be elevated in patients with severe periodontal disease. This increased concentration of IgA in GCF indicates the protective function of this immunoglobulin in periodontium and may also be helpful in identifying the individuals who are at a lower-risk of development of future periodontal disease 12.
IgM:
The mechanism of antibacterial action of IgM antibodies is primarily through agglutination, opsonization, and inhibition of attachment of pathogens to the host tissue. It also functions through neutralization and complement activation. It has been demonstrated that the GCF concentration of IgM significantly reduces following periodontal treatment 142.
Plasminogen activator (PA) and PA inhibitor-2 (PAI-2):
The PA system is of central importance in extracellular proteolysis. It acts in both physiological and pathological processes, such as tissue repair, tissue remodeling, local inflammatory reactions and neoplastic growth and invasion 143. Plasminogen is the key component of the PA system. The major function of ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Both plasmin activators and plasminogen activator inhibitors are present in GCF in inflamed gingiva as compared to healthy gingiva 146. In a study, levels of IL-1β, t-PA, PAI-2 and prostaglandin E2 in patients with periodontitis with or without rheumatoid arthritis and healthy individuals were evaluated. It was observed that there were higher levels of total amounts of t-PA in the periodontitis group than healthy individuals, but there were no statistically significant differences elucidated between other parameters 147. However, another investigation reported no significant differences in GCF levels of t-PA and PAI-2 between chronic periodontitis and aggressive periodontitis either before or after treatment 144.
Substance P and Neurokinin A:
Substance P is localized in sensory nerves that innervate blood vessels and is a member of the tachykinin family of neuropeptides. It is stored in the secretory granules of sensory neurons and their peripheral branches. The presence of substance P in GCF has been correlated with the presence of periodontal inflammation and reduction in periodontal inflammation as a result of effective periodontal treatment is associated with a reduction in the levels of substance P in GCF 148-150. Neurokinin A (NKA) is also a member of the tachykinin family of neuropeptides. As already stated, these molecules are involved in neurogenic inflammation 151. Following their release from nerve endings, these may get access to the GCF where they can be isolated and quantified 152.
Vasoactive intestinal peptide (VIP):
VIP is a 28-amino acid polypeptide which has a vasodilating action. It belongs to a glucagon/secretin superfamily. It has a modulatory effect on both natural and acquired immunity 153. In addition, VIP has been shown to be capable of regulating the production of both pro- and anti-inflammatory mediators 154, 155. VIP in the GCF has been found in increased quantities in periodontitis-affected than in clinically healthy sites. Also, the reduction in inflammation resulting from effective periodontal treatment was found to be associated with a reduction in the levels of VIP in GCF 156.
A study investigated the immunomodulatory effect of VIP. The effect of VIP on immune responses induced by P. gingivalis lipopolysaccharides (LPS) in vitro was investigated and the results showed that VIP (10−8 M) significantly (P < 0.05) inhibited TNF-α production by human monocytic THP1 cells stimulated with P. gingivalis LPS. In addition, VIP inhibited nuclear translocation of NFκB and c-Jun in a time-dependent manner but did not decrease the expression of CD14 receptors 157.
Platelet-activating factor (PAF):
PAF is a potent pro-inflammatory mediator. It is derived from a variety of cells including macrophages, thrombocytes, and lymphocytes 158. The primary function of PAF is that it promotes aggregation, chemotaxis, granule secretion, and oxygen radical generation from leukocytes and the adherence of leukocytes to the endothelium 159, 160. In addition, it also ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Neopterin:
Neopterin belongs to the class of pteridines which are biosynthetically derived from guanosine triphosphate (GTP). It is an early and a valuable marker of cellular immunity. The neopterin levels indicate the stage of activation of the cellular immune system which can be correlated to the pathogenesis of various diseases. It has been shown that neopterin level in GCF at periodontitis-affected sites is higher as compared to healthy sites 164. Another investigation reported that levels of neopterin in GCF increased according to the severity of periodontal inflammation and that its levels in GCF may be potentially useful as an indicator of periodontal inflammation and host response 165.
Cystatin:
Cystatins are inhibitors of cysteine proteinases and could play a protective and regulatory role under inflammatory conditions. They function as reversible, tight-binding inhibitors of cysteine proteases, and generally do not possess specific inhibitory activity to any particular cathepsin. Cystatin family comprises of three types. Type I cystatins (the stefins, stefins A and B), are cytosolic proteins which lack disulfide bridges. Type II cystatins are extracellular proteins containing two disulfide bridges and comprise of at least 14 members. Type III cystatins are kininogens which are large multifunctional plasma proteins, containing three Type II cystatin-like domains. Cystatin A is primarily responsible for GCF cystatin activity 166. An investigation done on Cystatin C concluded that its levels in GCF increase with periodontal disease progression to prevent further periodontal degeneration and decrease after treatment due to bone metabolic homeostasis 167.
CD14:
Originally described as a myeloid differentiation antigen, CD14 is a multifunctional, high-affinity receptor for endotoxins, LPS, and other bacterial wall components. This receptor is involved in the development and maturation of the innate immune system 168-171. It exists in membrane-bound and soluble forms. Many investigations have demonstrated a correlation between CD14 and the balance between cytokines released by Th1 and Th2-cells 172-174.
Studies have been done to find out any association between soluble CD14 (sCD14) levels in GCF and their potential relationship to periodontal conditions. In a study, sCD14 levels in GCF were determined in adult periodontitis patients. The authors reported a negative correlation between GCF sCD14 levels and probing depth 175. It has been proposed that sCD14 might play a protective role against disease 176.
Melatonin:
Melatonin is a methoxyindole, synthesized and secreted principally by the pineal gland. It is an amine of molecular weight 232Da, that is synthesized from tryptophan, an essential amino acid, via serotonin. It has antioxidant properties and plays a critical role in controlling inflammatory reactions. It acts as a scavenger to neutralize hydroxyl radicals, peroxyl radicals, and highly toxic peroxynitrite. The second mechanism of action is to activate endogenous enzymes that scavenge free-radicals. Studies have been done on salivary and GCF melatonin to determine its association with periodontal diseases. One study examined the levels of salivary and GCF melatonin in periodontal disease to find out any correlation between salivary and GCF melatonin with periodontal status. Melatonin concentrations in GCF were significantly less as compared to saliva. Melatonin concentration in GCF and saliva was inversely proportional to the clinical indices. It was concluded that melatonin may have a protective role against periodontal disease 177. Another study evaluated melatonin levels in the GCF and saliva of subjects with healthy periodontal tissues, plaque-induced gingival inflammation, Grade A/B (chronic) periodontitis and Grade C (aggressive) periodontitis. The results of the study revealed that melatonin levels in GCF and saliva decrease in diseased periodontal tissues, especially periodontitis 178. More clinical research is required to authenticate the association of melatonin levels and periodontal status.
Saliva
Saliva plays crucial role in the oral cavity in maintaining oral health and homeostasis. The primary functions of saliva are digestive and protective. The digestive functions include the formation of bolus by moistening the food, protection of the oral mucosa against mechanical damage and preliminary digestion of food through the presence of α- amylase and other enzymes. The protective functions include lubrication of the oral structures by mucins and its ability to act as a buffer (by bicarbonate, phosphates, and proteins) to maintain salivary pH around 7. The presence of calcium ions in saliva helps in the remineralization of enamel. The presence of various antimicrobial factors in saliva prevents microbial growth in the oral cavity. Other functions of saliva include speech articulation and maintenance of taste buds.
Formation and secretion of saliva
A healthy individual produces 500-1500 ml of saliva per day, at a rate of approximately 0.5 ml/min 179. The formation of saliva is under the control of the autonomic nervous system. The serous part of the glands is under the control of the sympathetic system and the mucous part is under the control of both parasympathetic and sympathetic systems. The quantity, viscosity, and ionic and protein concentrations of saliva are controlled by α-β adrenergic and cholinergic stimuli.
Saliva is produced by salivary glands viz. parotid glands, submandibular glands, sublingual glands and minor salivary glands. The parotids are the largest salivary glands with a wedge-shaped structure. The base of the wedge lies superficially and is covered by the fascia and the parotid capsule. The apex of the gland forms the deepest part. The gland is intimately associated with the peripheral branches of the facial nerve. The parotid gland pours its secretions into the oral cavity by a duct (Stensen’s duct) which opens into the oral cavity in a papilla opposite to the upper second molar. The submandibular gland is approximately half the size of the parotid gland. It pours its secretions into the oral cavity by a duct (Wharton’s duct) into the floor of the mouth underneath the anterior part of the tongue. The sublingual gland is the smallest of the paired salivary glands and is approximately one-fifth the size of the submandibular gland. The openings for the sublingual gland, or the sublingual caruncles, are located near the midline of the sublingual fold in the ventral tongue. The secretions of the major salivary glands are not identical. The secretions from parotids are primarily serous and from submandibular glands is a mixture of mucous and serous fluids. The secretion from the sublingual gland is primarily mucous.
The formation of saliva takes place in the acini where serous cells produce a watery seromucous secretion and mucous cells produce a viscous mucin-rich secretion. The source of this secretion is interstitial fluid derived from the blood in the capillaries which is modified during its passage through the salivary glands till it gets ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
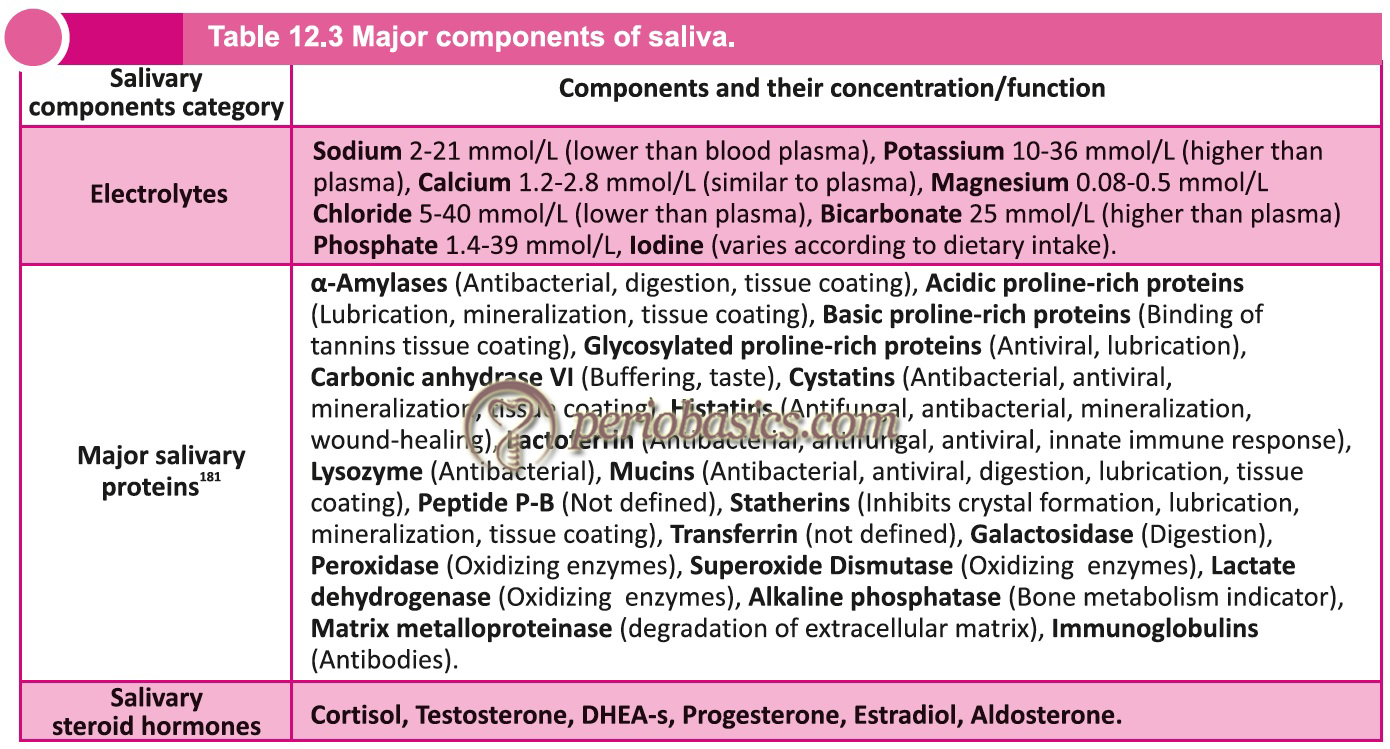
Composition of saliva
Around 99% of saliva is made up of water and the remaining part of saliva is composed of electrolytes, mucus, antibacterial compounds and various enzymes. Following table describes various components of saliva, other than water.
Review of literature on various components of saliva in periodontal health and disease
Saliva has been investigated for its various components and changes in their levels in periodontal health and disease. Salivary enzymes have a wide variety of effects on oral environment. The antioxidant enzymes are an important part of the host defense system in the oral cavity 182. It has been reported that salivary enzymes could affect the stability of dental implants 183, 184. The salivary enzymes may change the environment of the oral cavity which can predispose teeth for the development of dental caries and demineralization of the root surface 185, 186. Many salivary components and enzymes have been investigated to be used as biological markers to detect the course of periodontal problems and other possible diseases in the oral cavity. Following is their detailed description,
Antioxidants in saliva:
During the inflammatory process various reactive oxygen species (ROS) including oxygen-derived free radicals, such as superoxide (O2−), hydroxyl (OH) ions, nitric oxide, hydrogen peroxide, and hypochlorous acid (HOCl) are produced 187. These ROS are neutralized by various antioxidants in saliva such as superoxide dismutase, glutathione peroxidase, peroxidase, catalase, etc. The non-enzymatic antioxidants in saliva are uric acid, albumin, glutathione, vitamins A, C, etc. It has been proposed that in healthy individuals, there exists a balance between the oxidants and antioxidants in saliva whereas, in unhealthy individuals the oxidants have a higher level that can cause oxidative stresses 188.
Superoxide dismutase is the ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Glutathione reductase is an enzyme responsible for keeping glutathione in its reduced state, i.e., it converts the oxidized glutathione into reduced glutathione. Research done on the levels of this enzyme in periodontitis and healthy patients has revealed that chronic periodontitis patients have low levels of the protective antioxidant glutathione 193, 194. However, contradictory results have also been reported 195.
Studies have been done to investigate the total antioxidant capacity of saliva in periodontitis and healthy subjects. Moore et al. (1994) 196 observed no significant difference between the amount and activity of antioxidants in case and healthy control groups. On the other hand, Chapple et al. (1997) 197 reported that patients with periodontal diseases had a low total antioxidant status. Similar results were observed in other studies 198-200.
Liskmann et al. (2007) 201 observed that the total antioxidant status was lower in the peri-implant disease group than the healthy group. Kim et al. (2010) 192 found that the whole saliva antioxidant level increases after scaling. Due to variations in the results of studies regarding salivary levels of various antioxidants in health and periodontitis, more evidence is required to use them as biomarkers for periodontal disease.
Cytokines in saliva:
The source of salivary cytokines has been investigated and it seems to be GCF. In an investigation Ruhl et al.(2004) 202 estimated levels of Interleukin (IL)-1α, IL-6, IL-8, epidermal growth factor (EGF), nerve growth factor (NGF) and albumin in parotid, submandibular/ sublingual and whole saliva. The results of the study revealed that concentrations of IL-1α, IL-6, and IL-8 in the whole saliva were significantly higher than in major salivary gland secretions. They concluded that these cytokines were not derived from salivary glands, but probably from GCF. In another investigation, level of transforming growth factor (TGF)-β, IL-1α and tumor necrosis factor (TNF)-α were found significantly higher in the whole saliva as compared to saliva obtained from parotid gland 203.
Various investigations have been done to find any correlation between salivary cytokines and periodontal status. Studies have found elevated levels of IL-1β in periodontitis patients as compared to healthy volunteers 204-210 but others have reported contradictory results 211-213. One study reported a positive correlation between ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Research has also been done on cytokines related to bone cell activity such as osteocalcin, RANKL, and OPG (osteoprotegerin) because these markers may indicate bone loss during periodontal destruction 215, 216. However, variable results have been reported. One study has reported elevated levels of RANKL in saliva from periodontitis patient 217, whereas another study failed to find significant differences between RANKL levels in periodontitis as compared to controls 218. Similarly, some studies have reported lower levels of salivary OPG in periodontitis as compared to controls 213, 217 whereas some other studies found no evidence for such a correlation 204, 219, 220. Osteocalcin and osteonectin which are markers of bone metabolism have also been investigated in saliva taken from periodontitis and healthy individuals. Studies have reported variable results for their correlation with the periodontal status of the patient 221-225. A few studies have been done to analyze the correlation between salivary chemokines and periodontal breakdown. Two studies have reported a positive correlation between CCL3 (MIP-1α) levels and periodontitis 220, 226.
Lactate dehydrogenase (LDH):
As already stated, Lactate dehydrogenase (LDH), alkaline phosphatase (ALP), aspartate aminotransferase (AST), and alanine aminotransferase (ALT) are markers of cellular damage and inflammation. Many studies have demonstrated correlation between salivary levels of these enzymes and progressive periodontal disease 227-232.
Significantly higher levels of salivary LDH have been found in patients with rapidly progressive periodontitis 233. One study investigated the usefulness of various salivary biomarkers for screening of periodontal disease. Among the biochemical markers tested, salivary LDH levels had the highest sensitivity and specificity. However, in this study the serum levels of LDH were not investigated which can be an important factor affecting salivary levels of LDH 234. Another study investigated ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Alkaline phosphatase (ALP):
It is an intracellular enzyme present in most of the tissues and organs, particularly in the bones. It is one of the most important enzymes involved in the maintenance of periodontal ligament and root cementum. An increased ALP activity has been reported in the periodontal ligament due to renewal of the tissue as well as in pathological cases 237. The increased levels of this enzyme are indicative of alveolar bone destruction 238. This enzyme has been found in elevated concentration during active alveolar bone loss due to periodontitis, which establishes this enzyme as a potential salivary biomarker for periodontitis 239.
Aspartate aminotransferase (AST):
This enzyme is a good indicator of inflammation and cellular destruction. In a study done by Totan et al. (2006) 228, it was observed that there was a significant increase in salivary enzy-matic (aspartate aminotransferase, alkaline phosphatase and alanine aminotransferase) activities in periodontitis patients. In other studies done on GCF and saliva, it was observed that the improvement in periodontitis patients following perio-dontal therapy was associated with decreased AST levels 240, 241. It has also been shown that the levels of AST in saliva correlate with the depth of the periodontal pocket with higher AST levels associated with increasing pocket depth 227, 242.
β-glucuronidase:
As already discussed in GCF, β-glucuronidase is an enzyme found in neutrophil lysosomes. The primary function of this enzyme is the digestion of proteoglycans. The salivary levels of β-glucuronidase indicate neutrophil influx into GCF and its levels in saliva also correlate with the severity of the periodontal destruction 243, 244. Studies have demonstrated high level of salivary β-glucuronidase activity in patients with periodontitis 245. However, further research is required to establish β-glucuronidase levels in saliva as a biomarker for periodontal disease.
C-reactive protein (CRP):
The CRP levels are indicative of systemic inflammatory status. The relationship of elevated salivary and serum CRP levels in aggressive periodontitis cases has been demonstrated by Giannobile et al. (2009) 246. In another study, Azar et al. (2011) 247 compared CRP levels in the saliva of smokers and non-smokers. The results of the study showed a considerable increase in salivary CRP concentrations in smokers as compared to non-smokers. A study investigated salivary CRP levels in diabetic and non-diabetic patients with periodontitis. It was observed that the healthy control group had salivary CRP levels lower than the other two groups and there was no significant difference between the diabetic and non-diabetic patients with periodontitis 248. Another ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Matrix metalloproteinases:
The MMPs are the enzymes responsible for the degradation of ECM. There is limited data regarding relationship between salivary MMPs and periodontal status. One study investigated MMP-2 and MMP-9 in oral fluids of healthy subjects and periodontitis patients and the contributions of different oral cells to the enzyme production. The results of the study revealed that gelatinases are produced by various cells in the oral cavity and the amount of gelatinases is elevated during periodontal disease. After efficient periodontal treatment, the levels of these enzymes are reduced 60. Another study was done to investigate salivary matrix metalloproteinase (MMP-8) levels and gelatinase (MMP-9) activities in patients with type 2 diabetes mellitus. The study included 45 type 2 diabetic patients and 77 control subjects. The authors concluded that in uncontrolled diabetics, the increased oxidative burden in plasma is mainly by triggered neutrophils and they did not support the concept of generalized neutrophil dysfunction in unbalanced diabetes. Further, the authors conceded by stating that salivary MMP-8 levels in type 2 diabetes might be useful in monitoring periodontal disease in diabetes 251. More clinical research is required to outline the exact correlation of salivary MMP’s and periodontal disease progression.
Lactoferrin (LF):
The concentration of LF in unstimulated and stimulated saliva is 8.96 and 7.11 mg/l respectively. It is an important component of innate immunity. There is evidence that salivary LF levels reduce after surgical periodontal treatment in chronic periodontitis patients 140. A study demonstrated that the concentration of LF is strongly upregulated in mucosal secretions during gingival inflammation and is detected in a high concentration in saliva of patients with periodontal disease as compared with healthy patients 252. In another study, the LF levels were evaluated in healthy and chronic periodontitis patients. The subjects with chronic periodontitis showed higher concentrations of LF in stimulated whole saliva as compared to the healthy controls. Also, the salivary LF levels in chronic periodontitis patients correlated with probing pocket depth ≥ 6 mm 253. The salivary LF levels have been found to be increased in aggressive periodontitis patients 252, 254. However, it should be noted that studies concerning smoking and concentrations of LF in saliva have shown that LF levels tend to decrease in smokers 255-257.
Recently, a study was done to find out whether salivary LF levels in the GCF and saliva are different between HIV-infected and non-infected patients with chronic periodontitis. 28 HIV-infected and 10 non-infected patients were included in the study. Results demonstrated no significant differences in the GCF and saliva LF levels among HIV-infected and noninfected patients with chronic periodontitis 258.
Immunoglobulins:
Out of all immunoglobulin classes, IgAs which is produced by the plasma cells of the salivary glands are the most represented Ig type in the salivary fluid. Out of the two classes of IgA, IgA1 is predominant in serum while IgA2 is found in higher concentrations in external secretions, that is, tears, saliva, and milk 259. They provide immunity towards various oral bacteria. Lehner in 1969 260 proposed the ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Recently, a study was done to assess the level of salivary immunoglobulins and periodontal status in smokers and non-smokers. Unstimulated saliva was collected from 30 smokers and 30 non-smokers. IgA, IgG, and IgM were measured with the colorimetric immuno-enzymatic method. The results of the study revealed lower levels of salivary IgA, IgG, and IgM and a worse periodontal condition in smokers than in non-smokers, indicating that deteriorated periodontal status in smokers was associated with lowering of the host’s defense due to a decrease in the quantity of Ig’s in salivary fluid 269.
Lysozyme:
This enzyme has antimicrobial properties. It causes cleavage of chemical bonds in the bacterial cell wall, resulting in disruption of bacterial cell wall. It works on both Gram-negative and Gram-positive microorganisms. The Gram-negative bacteria are more resistant to lysozyme due to the presence of the external lipopolysaccharide layer. It has been reported that patients with low levels of salivary lyzozyme are more susceptible to plaque accumulation, which is considered as a risk factor for periodontal disease 270. In a study, amounts of antibacterial proteins cystatin SA, cystatin C and lysozyme in saliva were compared between healthy persons and subjects with periodontitis. The results of the study showed that the concentration of all these antibacterial proteins in periodontitis patients was significantly lower than the healthy subjects 271. It has been shown that patients with insulin-dependent diabetes 272 and HIV-infected individuals 273 show a significant decrease in salivary lysozyme concentration as compared to healthy individuals.
Histatins:
Histatins are antimicrobial proteins in saliva, primarily secreted from parotid and submandibular glands. The function of theses proteins is neutralization of the endotoxic lipopolysaccharides located in the membrane of Gram-negative bacteria. In human saliva, at least 12 histatin-like peptides have been identified. Out of all histatins, histatins 1, 3 and 5 are most abundant in parotid saliva. Histatin 5 has also been extensively investigated because of its potent fungicidal properties 274. Along with antibacterial activity, there are ……. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book….
Defensins:
Defensins participate in both adaptive and innate immune response. The defensins can be divided into two families: α and β defensins. In humans, there are six α-defensins and four β-defensins. α-defensins are produced by PMNs. These are involved in various functions such as, they increase the production of pro-inflammatory cytokines (tumor necrosis factor (TNF) and IL-1) and decrease the production of IL-10 by monocytes. These are also capable of enhancing or suppressing the activation of the classical pathway of complement system.
Human β-defensins (HBDs) are small cationic peptides primarily produced by epithelial cells. They have bactericidal action by creating pores into the bacterial membranes of Gram-negative and Gram-positive bacteria and hence, play an important role in the oral cavity as the first-line of defense against bacterial infection. In the oral cavity, epithelial cells express three HBDs: HBD-1, HBD-2 and HBD-3 280, 281. HBD-4 is expressed by genital associated organs, thyroid, lung, and kidney. In a study, salivary levels of HBD-2 protein concentration in healthy individuals and patients with gingivitis and chronic periodontitis were investigated. The results of the study revealed that salivary HBD-2 protein concentration was higher in patients with chronic periodontitis as compared with healthy individuals or patients with gingivitis. However, the protein concentrations did not relate to the frequency of periodontopathogens 282. It has been proposed that salivary levels of defensins can alter in oral diseases and these can be useful markers for risk assessment 283.
Conclusion
Extensive research has been done on GCF and saliva in search of reliable markers for monitoring periodontal disease activity. Various components of GCF and saliva have been investigated to detect the present status of the periodontal condition and the probable future status. Analysis of GCF or saliva provides us a non-invasive access to the periodontium for monitoring its state of health. Various chairside diagnostic kits have been introduced which can detect specific molecules in GCF or saliva and provide us the result in a shorter duration of time. However, we are still far from an ideal or near ideal biomarker in GCF or saliva, which can provide accurate information regarding the present status of the periodontium and predict its future status.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.