Introduction to dental cementum
Cementum is an avascular mineralized mesenchymal tissue covering the entire root surface. Although, it is an integral part of the tooth, but functionally it is a component of the periodontium. It was first described in 1835 329 and since then it has been studied extensively. It functions as the site of attachment for principal collagen fibers (Sharpey’s fibers) of PDL. Cementum has unique properties such as, it is avascular and lacks innervation, it does not express parathormone receptors (as do osteoblasts), so does not undergo remodelling as bone and its thickness goes on increasing throughout life 330, 331. The resorption of the cementum is less as compared to bone, so during orthodontic tooth movement, bone remodeling takes place with minimal effect on root cementum 332.
Development of cementum
During tooth formation, the inner enamel epithelium of the dental organ differentiates into enamel producing cell, ameloblasts. But, the cells of the inner epithelium of the apical extension of the enamel organ, the epithelial root sheath, do not differentiate into ameloblasts. Instead, the cellular interactions of these cells with neighboring ectomesenchyme results in the differentiation of cells from the dental papilla into odontoblasts which deposit pre-dentine. Immediately after the formation of pre-dentin, an enamel-like material is deposited on its surface which is considered to be an initiating factor for the differentiation of cementoblasts. Now, cells from the dental follicle differentiate into cementoblasts and start depositing cementum on the surface of dentine. With the disintegration of the epithelial root sheath, the cells from the dental follicle directly come in contact with the dentine where they start depositing cementum.
Classification of cementum
The cementum has been classified according to various factors including, presence or absence of cells, the nature and origin of the organic matrix or combination of both.
Depending on the presence or absence of cells:
- Cellular cementum.
- Acellular cementum.
Cementum has been traditionally classified into cellular and acellular, depending on the presence or absence of cementocytes in its structure. The acellular cementum is the initially formed cementum found on the cervical portion of the root. Cellular cementum is found on the apical portion of the root and is deposited when the tooth enters its functional stage (Table). However, this arrangement is not always present and deviations do exist. Sometimes several alternate layers of these two variants are present, referred to as “mixed stratified cementum” (multiple interposed layers of acellular extrinsic fiber cementum and cellular intrinsic fiber cementum). The acellular cementum is generally formed before tooth eruption and prior to teeth reaching the functional occlusion. It is also known as “primary cementum”. This cementum contains comparatively fewer collagen fibers which are placed more or less perpendicular to the dentinocemental junction. Subsequently, when teeth achieve occlusal contacts, cementum formed is known as the “secondary cementum”. It is characterized by the presence of dense collagen matrix. It may be cellular or acellular 333.

Differences between cellular and acellular cementum
| Acellular cementum | Cellular cementum |
|---|---|
| Generally formed before tooth eruption and prior to teeth reaching the functional occlusion. | Generally formed after tooth achieves occlusal contacts. |
| It does not contain cells. | It contains lacunae and canaliculi containing cementocytes and their processes. |
| Border with dentine is not clearly demarcated. | Border with dentine is clearly demarcated. |
| Rate of development is relatively slow. | Rate of development is relatively fast. |
| Incremental lines are relatively close together. | Incremental lines are relatively wide apart. |
| Pre-cementum layer is narrow. | Pre-cementum layer is wide. |
| Usually more calcified. | Usually less calcified. |
| Sharpey's fibers are the main component and insert at right angle onto the root surface. | Sharpey's fibers occupy smaller proportion and are not the main component. |
Depending on the nature and origin of the organic matrix:
- Extrinsic fiber cementum.
- Intrinsic fiber cementum.
There can be two sources of the organic matrix for the formation of cementum: fibers from the PDL or from the cementoblasts. When the fibers are derived from PDL, they are referred to as extrinsic fibers and when these fibers are derived from cementoblasts, these are referred to as intrinsic fibers. The extrinsic fibers or the Sharpey’s fibers are inserted into the cementum in the same direction as that of the principal fibers i.e. perpendicular or oblique to the root surface. The intrinsic fibers run parallel to the root surface and are oriented almost perpendicular to the extrinsic fibers. When both extrinsic and intrinsic fibers are present simultaneously, the cementum is then referred to as mixed fiber cementum.
Depending on the time of formation, presence or absence of cells and on the nature and origin of the organic matrix:
This is the most commonly used classifications to describe various types of cementum. In this classification following types of cementum have been described,
- Primary acellular intrinsic fiber cementum.
- Primary acellular extrinsic fiber cementum.
- Secondary cellular intrinsic fiber cementum.
- Secondary cellular mixed fiber cementum.
- Acellular afibrillar cementum.
Primary acellular intrinsic fiber cementum:
This cementum is formed before the formation of the PDL, hence, the collagen fibers in its matrix are derived from the cementoblasts. When the thickness of this cementum reaches 15-20 μm, the fibrous fringes of this cementum come in contact with the PDL fiber bundles.
Primary acellular extrinsic fiber cementum:
This cementum is characterized by the presence of densely packed bundles of Sharpey’s fibers which are derived from PDL. It is usually found in the cervical third of the root, but may also be found further apically. Its thickness varies from 30-230 μm. This cementum is acellular and does not contain cementocytes in its matrix. As its formation occurs after the formation of PDL, it becomes a principal attachment apparatus for PDL and cementum. This type of cementum is more mineralized than other types of cementum.
Secondary cellular intrinsic fiber cementum:
This cementum is formed of collagen fibers which are almost entirely derived from the cementoblasts. It must be noted here that the.…….. Content available in the hard copy of the website……… Content available in the hard copy of the website……………… Content available in the hard copy of the website………
Secondary cellular mixed fiber cementum:
This cementum contains both Sharpey’s fibers derived from the PDL and fibers from the cementoblasts. This cementum forms the bulk of the secondary cementum. With light microscope, a lamellate structure can be seen in this cementum with the presence of cementoid on its surface. It is variably present on the root surface depending upon the functional state of the tooth. The cells in this type of cementum are placed haphazardly and depending upon the distance from the surface of cementum their viability differs. The cells, which are closer to the cementum surface get their nutrient supply from the PDL and are viable. As we go into the deeper layers, these cells loose intracellular organelles and ultimately die. Cementocytes possess cellular processes in the canaliculi but there is no evidence which suggests them forming a syncytium. On different areas on the root surface, the thickness of this type of cementum varies from 100-1000 μm.

Acellular afibrillar cementum:
As the name indicates, this type of cementum neither contains cells nor collagen fibers. It is a product of cementoblasts and is found only in the cervical areas of the tooth. Its distribution varies from tooth to tooth and CEJ of the same tooth. The thickness of this cementum in humans varies from 1-15 μm. Under light and electron it appears as a non-homogenous matrix composed of multiple calcified layers without collagen fibers. It plays no role in tooth attachment and is considered as a developmental anomaly.
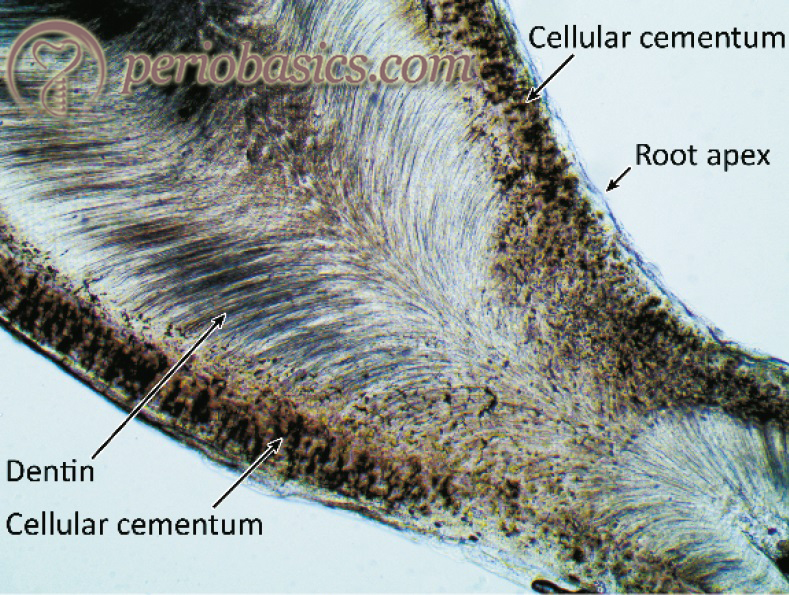
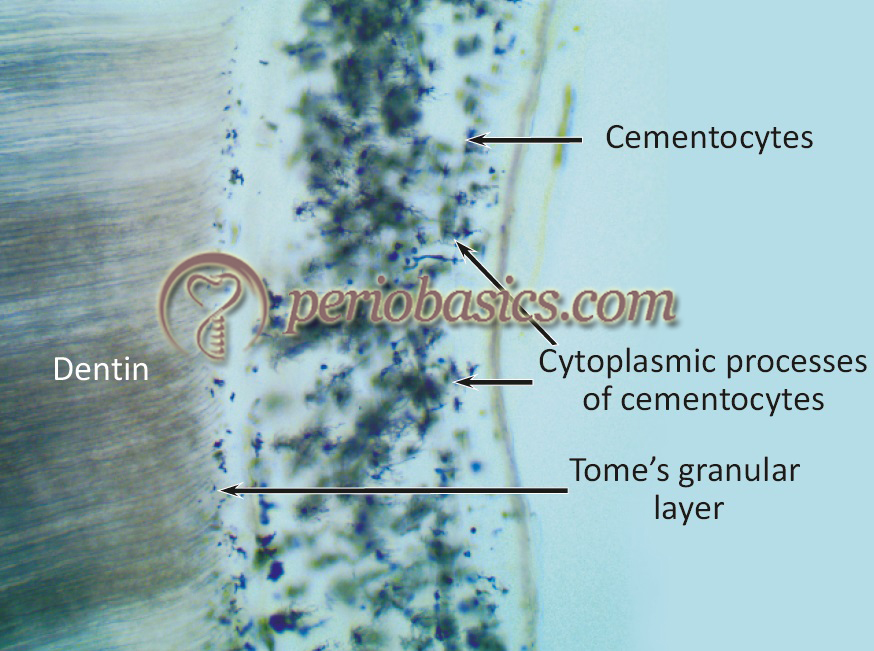
Microscopic features of cementum
Microscopically, the acellular cementum appears relatively structureless. In the apical portion of the tooth, the most common presentation is that of cellular cementum covering the acellular cementum. However, variations can be seen. The difference between that rate of cementum formation in cellular and acellular cementum can be observed by the presence of a precementum layer and more widely spaced incremental lines in the cellular cementum. The cementocytes are observed inside spaces known as lacunae. In the ground section of the cementum, the cellular contents are lost and the empty spaces appear dark with air and debris filling them. The arrangement of cementocytes in the cementum is quite different from that of osteocytes in bone. As already stated the cementocytes are more widely dispersed and more randomly arranged with varying degree of spaces between them. The canaliculi of cementocytes are preferentially oriented towards the PDL, which is their primary source of nutrition.
Incremental lines are observed in cementum, which reflects the deposition of cementum in an irregular rhythm. These lines are a result of differences in the degree of mineralization. These lines are closer in acellular cementum as compared to cellular cementum.
Composition of cementum
Cementum is composed of 50% organic and 50% inorganic components. The organic part is primarily composed of 95% of collagen Type I and 5% of collagen Type III 330. Electron microscopic examination shows densely packed collagen fibrils surrounded by granular matrix 333-338. Most of these fibrils are oriented more or less perpendicular to the root surface 339.
Organic components other than collagen include two major glycoproteins, bone sialoprotein (BSP) and osteopontin (OPN) 340. These are mainly present in acellular afibrillar cementum and cellular intrinsic fiber cementum. They are formed during the development of the tooth and have been proposed to play a major role in the differentiation of cementoblast progenitor cells to cementoblast 341. These glycoproteins have arginine-glycine-aspartic acid (RGD) adhesion domain which participates in cell migration and adhesion 342, 343. Other components of the organic matrix of the cementum are osteonectin, osteocalcin, and laminin.
The organic portion of the cementum also contains important polypeptide growth factors such as, bone morphogenetic proteins (primarily BMP-2, -3 and -4), α and β fibroblast derived growth factor (FGF), platelet-derived growth factor (PDGF), transforming growth factor (TGF) beta and parathyroid hormone (PTH) 341, 344, 345. Molecular factors specifically present in cementum are cementum growth factors (CGF), insulin-like growth factor (IGF)-1 isoform 346 and cementum attachment protein (CAP). These molecular factors are responsible for cell migration and mineralization of cementum 347, 348. It has been shown that cementum also contains chemokines and integrins, which promote differentiation and proliferation of some periodontal cell types 349.
The inorganic components of the cementum are similar to that of other calcified tissues such as bone, dentin, and enamel. The principal mineral component of cementum is ..… Content available in the hard copy of the website……… Content available in the hard copy of the website……………… Content available in the hard copy of the website……..
Cementum and enamel junction
The thickness of cementum reduces in the coronal direction to end in the vicinity of the cervical region. The cementum and enamel relation is variable. In 60-65% of instances, cementum overlaps the cervical enamel. In around 30% of cases, the cementum touches but does not overlap the enamel. In 5-10% of instances, there remains a gap between the cementum and enamel, leaving exposed dentin. All these relationships may exist on a single tooth.

Functions of cementum
There are three major functions of cementum. Firstly, it provides attachment to Sharpey’s fibers of the PDL, thus attaching the tooth to the alveolar bone. Secondly, it is involved in maintaining the normal PDL space. Finally, it serves as a medium through which the damage to the root surface is repaired.
Hypercementosis:
It is an abnormality associated with the formation of excessively thick cementum on the root surfaces, which may affect an individual tooth or multiple teeth. The generalized hypercementosis may be a hereditary condition and has been described in conjunction with Paget’s disease 356. The cementum thickening is more marked in the apical third of the tooth. In localized hypertrophy, spur or prong-like projections of cementum can be seen. These are usually seen in teeth subjected to greater stress. Teeth that are not in function have thickened cementum around the entire root surface with the reduced number of Sharpey’s fibers.
Cementicles:
These are small globular masses of acellular cementum found within the PDL. They are usually less than 0.5 mm in diameter. It has been proposed that they originate from foci of degenerating epithelial cell rests of Malassez in PDL 357. These may lie free in the PDL space (free cementicles) or may be attached (attached cementicles) to the radicular cementum. The attached cementicles eventually get incorporated into the cementum (interstitial cementicles). There is no significant clinical significance of the cementicles until they are exposed to the oral environment, where they may act as plaque accumulation factors.
Permeability of cementum
In health, cementum has a porous matrix because of which it is permeable to water and certain inorganic ions. However, on a diseased root surface, cementum is permeable to salivary organic components and plaque bacterial byproducts. It has been shown that on a plaque-associated root surface, the bacterial products are present up to the depth of 10 to 12 μm 358. The bacterial lipopolysaccharides have been detected at a distance of 70 μm from the periodontally diseased root surface 359. Another factor associated with the permeability of cementum is bacterial penetration. Bacteria invading the cementum have been demonstrated in studies 358. It has been proposed that the bacteria penetrating the root cementum can act as a reservoir of periodontopathogenic bacteria 360. The permeability of cementum reduces with age 361.
Age changes in cementum
The cementum deposition occurs at a linear rate throughout life 362. Like bone, cementum is a dynamic tissue and it responds to the occlusal forces and orthodontic forces. The cementum is thickest in the apical areas of teeth and in furcation areas of multi-rooted teeth 363. It has been proposed that the thickness of cementum is increased by tensional forces 364. However, no clear-cut relationship between functional stress and cementum thickness has been demonstrated. The incremental lines in cementum demonstrate the changes in the rate of cementum deposition during different time periods. With increasing age, the thickness of cementum increases. It has been shown to triple in thickness between the ages of 20 and 60 years 365. This factor can be used in the determination of age in forensic dentistry. The thickness of cementum on the distal root surfaces is more than on the mesial root surfaces 366. Continuous cementum deposition is essential for the mesial drift of the teeth as well as the compensatory eruption of teeth accounting for the occlusal wear.
Changes in cementum associated with periodontal involvement
Many changes are observed in the cementum of a periodontally involved root surface. The main changes observed are breakdown of dentogingival fibers, loss of collagen fiber cross banding and dissolution of inorganic content of the cementum 367, 368. Areas of hyper-mineralization in cementum have been demonstrated by chemical 352, 369, micro-radiographic 368, 370-372, and SEM-microprobe 350 investigations. However, some investigators did not observe any changes in the cementum mineralization on a diseased root surface 373, 374. A detailed description of changes in cementum exposed to oral environment due to pocket formation has been given in “Periodontal pocket”.
Cementum resorption
As already stated, PDL is the most important factor which prevents root resorption. It has been proposed that cells derived from PDL are not only responsible for osteogenesis and osteoclasis, but also for fibrogenesis and fibroclasis in the ligament itself, as well as for cementogenesis and cementoclasis on the root surface 266. Permanent teeth do not undergo physiological resorption as do the primary teeth. However, areas of cementum resorption at the microscopic level can be seen. In general, areas of cementum resorption increase with age. One study showed that 90.5% of teeth showed areas of cementum resorption in adult teeth 375. Bay like concavities can be seen under the microscope in the areas of cementum resorption. Adjacent to areas undergoing resorption, multinucleated giant cells, and mononuclear cell are generally seen.
Many factors such as inflammation, mechanical trauma, trauma from occlusion 376, orthodontic tooth movement 377-379, periapical pathology and pressure from the malaligned erupting tooth are associated with the resorption of cementum. Teeth without a functional antagonist and replanted/ transplanted teeth 380, 381 may also show areas of cementum resorption. Systemic diseases associated with cementum resorption include hereditary fibrous osteodystrophy 382, Paget’s disease 383, hypothyroidism and calcium deficiency 384.
The repair of cementum occurs by……. Content available in the hard copy of the website……… Content available in the hard copy of the website……………… Content available in the hard copy of the website…….
Conclusion
Cementum is a very important component of the periodontium. Recent evidence demonstrates that cementum plays an important role in periodontal regeneration. However, many aspects of dental cementum still need to be explored. In the above discussion, we studied various anatomical, physiological and also the pathological aspects of dental cementum. A detailed description of pathological changes that occur in cementum in periodontitis associated teeth has been given in “Periodontal pocket”.
References
References are available in the hard copy of the website.