Introduction to diabetes
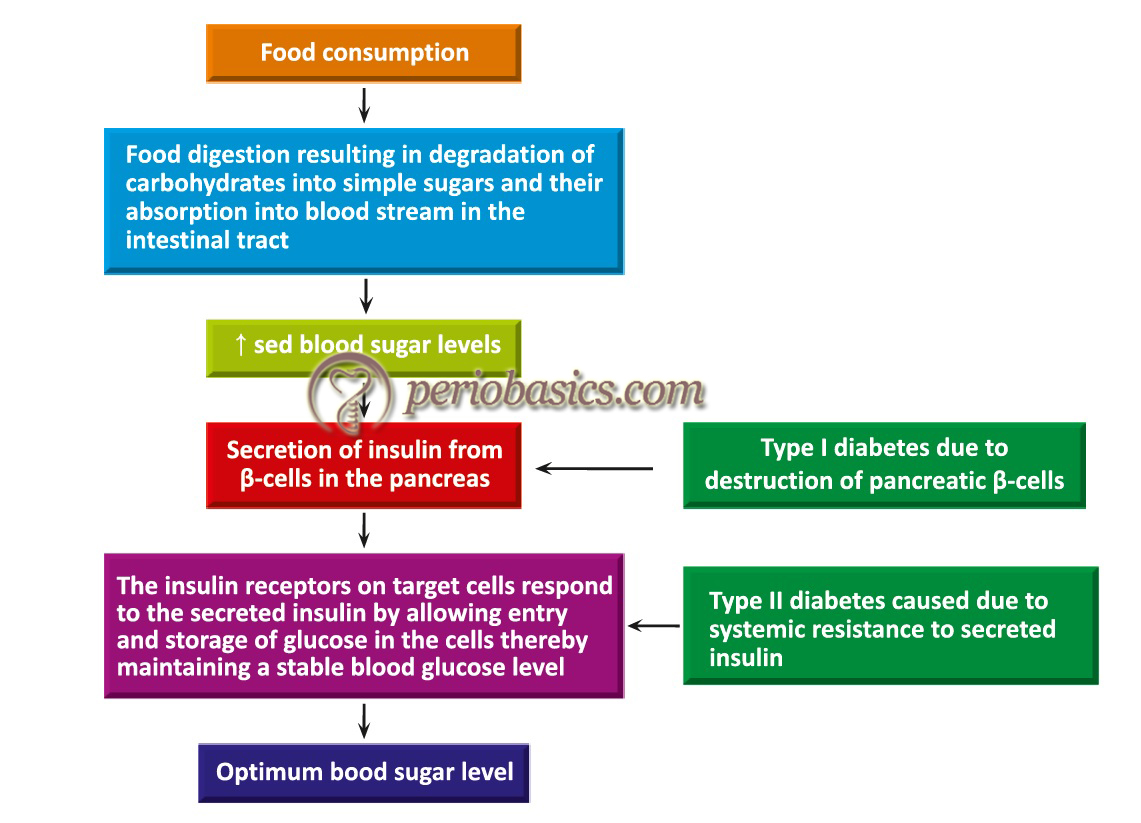
Diabetes mellitus is the most common endocrine disorder, characterized by an inability of the body’s cells to utilize glucose. According to World Health Organization (2014), 422 million adults are living with diabetes worldwide 1. Diabetes has been classified into two types, type 1 and type 2 diabetes. Type 1 diabetes results from cellular mediated autoimmune destruction of pancreatic β-cells, usually leading to total loss of insulin secretion. It constitutes about 5-10% of all cases of diabetes but accounts for more than 90% of diabetes cases in young people less than 25 years old. Type 2 diabetes, which is also known as non-insulin dependent diabetes, results from insulin resistance, which alters the use of endogenously produced insulin at the target cells 2, 3. type 2 diabetes constitutes 90-95% of all diabetes cases.
Evidence in support of periodontitis and diabetes relationship
In diabetes, the function of immune cells, including neutrophils, monocytes, and macrophages is often altered. Various neutrophil functions like adherence, chemotaxis and phagocytosis are changed, inhibiting an adequate defense against microorganisms in periodontal infections, thereby significantly increasing the destruction of the periodontal tissues 4. Clinical studies have demonstrated a higher prevalence of periodontitis in diabetic patients 5-7. The risk of periodontitis is increased by approximately three-fold in diabetic individuals as compared to non-diabetic individuals 2. The US National Health and Nutrition Examination Survey (NHANES) III, demonstrated that adults with a glycated hemoglobin (HbA1c) level of >9% had a significantly higher prevalence of severe periodontitis than those without diabetes after controlling for age, ethnicity, education, sex and smoking 8. In a study done on the Pima Indians, the incidence and prevalence of periodontal disease were determined in 2,273 subjects 15 years of age or older. The prevalence of periodontitis was 60% in subjects with diabetes and 36% in those without diabetes 9. A large cross-sectional study showed that diabetic patients were twice as likely as nondiabetic subjects to have an attachment loss 10. Studies done on HbA1c assay in diabetic patients have shown that the combination of scaling and root planing with systemic doxycycline therapy is associated with an improvement in the periodontal status and is also accompanied by a significant improvement in glycemic control 11-13.
On the other hand, periodontitis has been shown to worsen the diabetic status of the patient. It has been shown that severe periodontitis is associated with increased risk of poor glycemic control (HbA1c >9.0%, 75 mmol/mol) 14. A bi-directional relationship between periodontal disease and glycemic control with each disease having a potential impact on the other has been emphasized by many researchers 15-17. Longitudinal studies have shown that the patients with severe periodontitis are more likely to ………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
It has also been reported that smoking increases the risk of periodontal disease by nearly 10 times in diabetic patients 20. Patients with advanced periodontitis have been shown to have increased prevalence of diabetes-related complications, including cardiovascular complications, retinopathy, neuropathy and proteinuria 20-23. A longitudinal study investigated the impact of periodontitis on deaths from cardiovascular complications and diabetic nephropathy in Pima Indians with type 2 diabetes. After adjustment for age and gender, the death rate was calculated as 3.7 for those with no/mild periodontitis, 19.6 for those with moderate periodontitis and 28.4 for those with severe periodontitis. Furthermore, after adjustment for known confounders, the risk of cardiorenal mortality in patients with severe periodontitis was found to be 3.2 times more as compared to reference groups, which consisted of the patients with no periodontitis and the combined group of patients with mild and moderate periodontitis 24.


The proposed pathways of diabetes affecting periodontitis
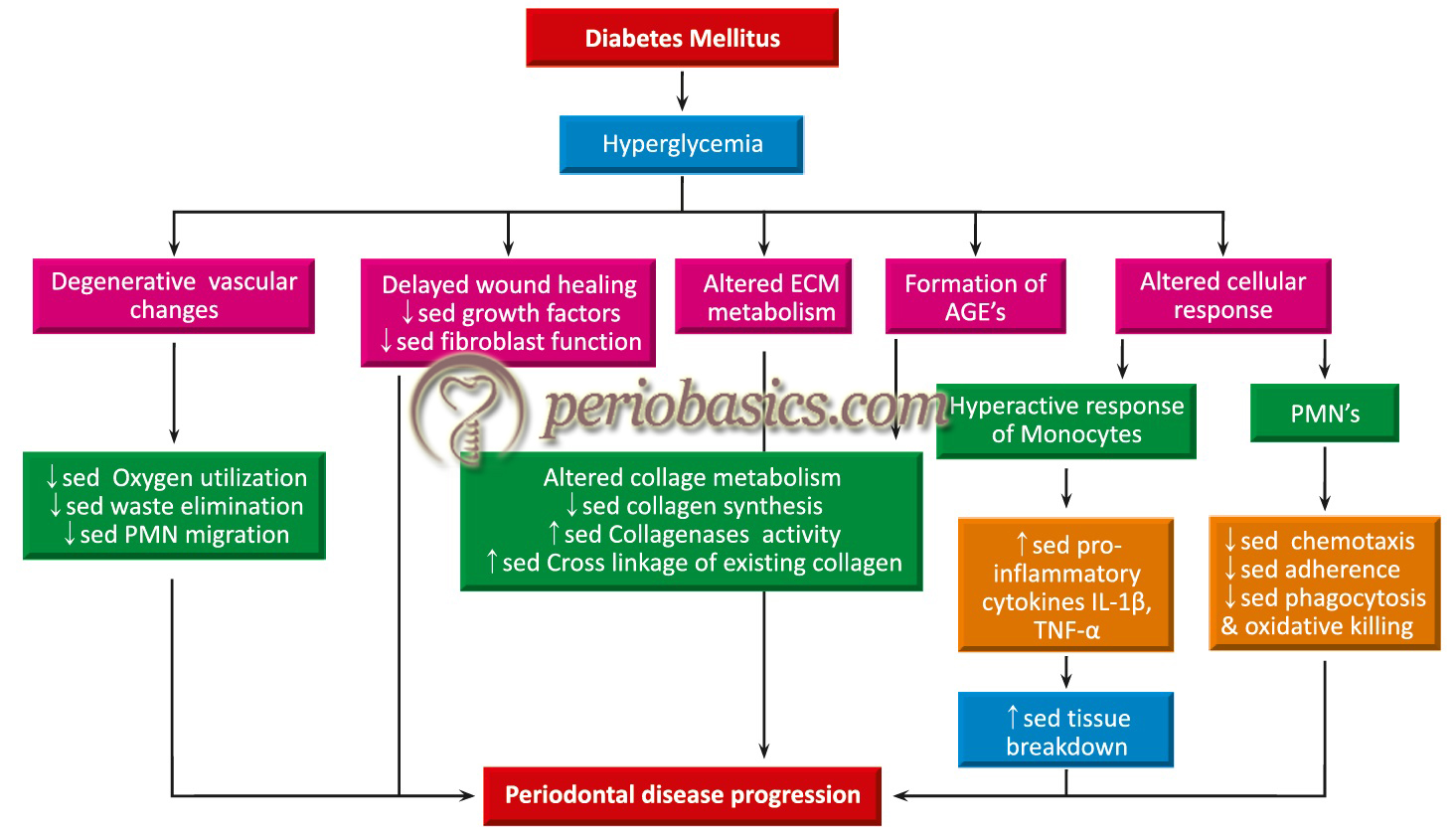
Various mechanisms have been proposed which explain how diabetes worsens the periodontal disease status. The complications of diabetes have been well described as diabetic retinopathy, nephropathy, neuropathy, macrovascular diseases and altered wound healing. Most of the microbiological investigations done on the subgingival microflora of diabetic and non-diabetic patients do not indicate any significant differences in the subgingival micro-organism species 25-27. This fact indicates that the increased prevalence and severity of periodontitis in diabetic patients may be due to differences in host response factors. The clinical signs of gingivitis in diabetic patients, summarized in a review 28 are given in the following table,
| Signs of gingivitis and periodontitis in diabetic patients. |
|---|
| Enlarged velvety-red gingival tissues that bleed easily. |
| Vascular changes that can give the gingivae a distinct purple /bluish hue. |
| Multiple periodontal abscesses. |
| Mobile teeth, indicating bone loss. |
| Proliferative tissue at the gingival margin. |
| Inflammation spreading through the attached gingiva. |
| Delayed wound healing following oral surgical procedures. |

Let us discuss the changes in the host immune response in diabetic patients,
Effects of diabetes on cellular response and tissue homeostasis
The inflammatory cells such as neutrophils, monocytes, and macrophages play an important role during host response. In diabetic patients, the response of these cells is altered 26.
Impairment in neutrophil function:
In diabetic patients, chemotaxis, adherence, phagocytosis, and microbial killing functions of neutrophils are impaired. This leads to the impairment of bacterial killing by neutrophils in the periodontal pocket and significantly increase periodontal destruction 4, 29. The decreased chemotactic activity of neutrophils in diabetic patients was shown for the first time by Mowat and Baum (1971) 30. The exact mechanism of decreased chemotaxis of neutrophils in diabetics is not well understood, however, it has been proposed that impairment of rolling and adhesion of leukocytes to the endothelial cells in diabetics is responsible for their defective chemotaxis 31. The neutrophil rolling and adhesion to the endothelial cells is mediated by the expression of ligands such as, intercellular adhesion molecule-1 (ICAM-1) on endothelial cells. Glycoproteins of the CD11/CD18 complex (β2 integrins) expressed on leukocytes interact with these ligands during transendothelial migration.
It has been proposed that downregulation of these adhesion molecules, that regulate leukocyte recruitment during the course of inflammatory processes, may also be a possible mechanism of defective neutrophil chemotaxis in diabetics 32, 33. The neutrophil function may also be impaired due to reduced glucose-6-phosphate dehydrogenase (G6PDH) activity. This is a rate-limiting enzyme in the pentose phosphate pathway. The neutrophils, macrophages, and lymphocytes ………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………
As already stated, the phagocytotic function of neutrophils in diabetics is also impaired. Nolan et al. (1978) 38 reported that in diabetic patients with fasting blood glucose value of more than 200 mg/dL, granulocytes had impaired ability to engulf the opsonized Staphylococci. Furthermore, it has been demonstrated that reduction of blood glucose levels by insulin treatment of diabetic patients 39 or rats 40 significantly correlated with the improvement of neutrophil phagocytosis capacity.
Neutrophils kill bacteria by building an oxidative burst. The respiratory burst requires the formation of NADPH. In neutrophils, pentose phosphate pathway is responsible for the formation of NADPH and ribose-5-phosphate for fatty acid and nucleotide synthesis, respectively 41. NADPH is important for NADPH oxidase and glutathione activity in neutrophils 42, 43. In diabetic patients, NADPH production is decreased, which leads eventually to compromised neutrophil function. The lowering of blood glucose levels by insulin treatment has been reported to have a significant correlation with the improvement of phagocytotic capacity of neutrophils 39, 44.
Altered monocyte-macrophage function:
The monocyte-macrophage function in diabetics has also been shown to be altered. The monocytes isolated from the peripheral blood samples from diabetic patients have been shown to secrete significantly more prostaglandin E2 in response to bacterial endotoxins than those without the disease 45. The gingival crevicular fluid (GCF) samples from diabetics have shown to have a higher concentration of cytokines (IL-1β, PGE2, TNF-α) as compared to non-diabetic subjects, which have been proposed to be derived from monocyte-macrophage lineage cells. This hyperinflammatory response is thought to be a result of advanced glycosylation end products (AGE) and their receptors (RAGE) interaction on monocytes and macrophages. This hyperactive cell phenotype releases excessive cytokines, thus resulting in more connective tissue damage. It has been proposed that AGE-RAGE binding on macrophage surfaces may alter macrophage phenotype, causing dysregulation of macrophage cytokine production and increased inflammatory tissue destruction and alveolar bone loss 46. Furthermore, it has also been proposed that this altered scavenging function of macrophages is one of the reasons for the delayed wound healing in diabetics 47.
Raised levels of monocyte chemoattractant protein (MCP)-1 in ………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………
Collagen homeostasis:
Collagen is the major structural protein in the periodontium. The collagen synthesis, maturation, and general turnover are greatly affected in diabetes. In diabetic patients, changes in collagen synthesis, maturation, and homeostatic turnover have been demonstrated. Under hyperglycemic conditions, the ………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………
In addition to reduced collagen and glycosaminoglycan synthesis, the newly formed collagen is susceptible to degradation by MMPs such as collagenase, which are elevated in diabetic tissues, including the periodontium 51, 52. The newly formed collagen fibers get degraded by MMP’s but the existing fibers become highly cross-linked, in the presence of AGEs, decreasing their solubility 53. These result in an abnormal collagen turnover and the collagen homeostasis is disturbed.
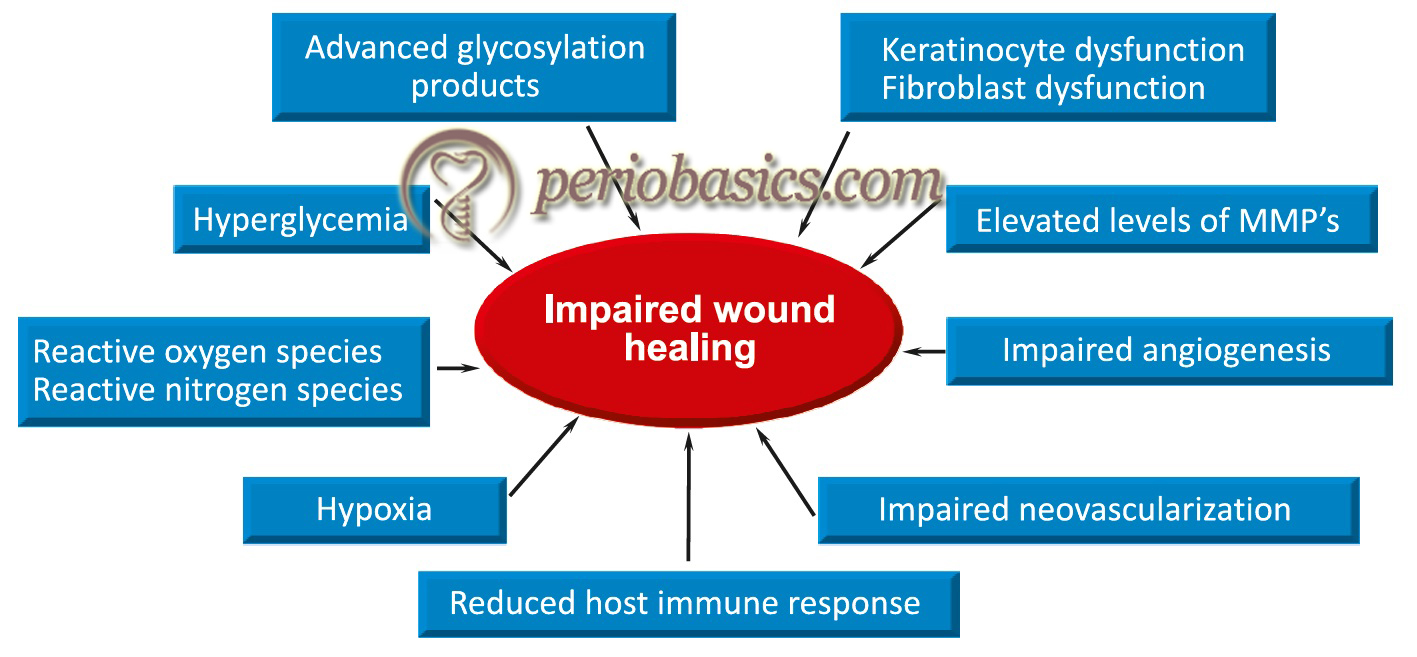
Altered wound healing:
This is one of the most common complications in diabetic patients. Increased levels of glucose in the GCF lead to hinder-ing of fibroblast function during wound healing. The attachment and spreading of these cells are critical to wound healing and normal tissue turnover 54. Growth factors are important for wound healing. Studies have shown that production of growth factors, such as platelet-derived growth factor, transforming growth factor-β and fibroblastic growth factor, is significantly reduced in diabetic patients 55, 56.
Role of advanced glycosylation end products:
In the hyperglycemic state, the advanced glycosylation end products (AGEs) are formed. These affect the vasculature by stimulating arterial smooth muscle cell proliferation and increasing the thickness of the vessel wall. Abnormal cross-linkage of AGEs modified collagen in the basement membrane causes abnormal degradation of these proteins, leading to thickening of the basement membrane. AGEs activate a receptor known as ”receptor for AGEs” (RAGE) found on the surface of smooth muscle cells, endothelial cells, neurons, and monocytes/macrophages, resulting in increased cytokine production by these cells 57. Studies have indicated an increase in pro-inflammatory cytokine levels in GCF in diabetic patients 58, which can be related to the above-stated action of AGEs.
As already stated, AGEs cross-link with basement membrane collagen and alter the vessel wall structure. The circulating low-density lipoproteins (LDL) becomes cross-linked to this AGE-modified collagen and contributes to atheroma formation. Furthermore, in small blood vessels, the cross-linking of AGEs with collagen fibers results in increased basement membrane thickness and compromised transport of nutrients across the membrane 59, 60.
AGEs are also associated with increased expression of various genes regulated by the transcription factor, nuclear factor-κB (NF-κB) 61. It alters the phenotype of the monocyte/macrophage and ………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………
Increased oxidative stress:
Hyperglycemia increases oxidative stress, which contributes to the cellular and extracellular damage. In addition, antioxidant mechanisms are diminished in diabetic patients, which may further augment oxidative stress 66, 67. The AGEs formed in the diabetic patient have been associated with enhanced oxidative stress 68, 69 and subsequent expression of endothelial vascular cell adhesion molecule (VCAM)-1 70. These changes further enhance the destructive process and contribute to the connective tissue destruction.
Effect on osteoblastic and osteoclastic function:
Under normal conditions, there is a critical balance between the osteoblastic and osteoclastic activity, maintaining the normal bone turnover. However, in a hyperglycemic state, there is inhibition of osteoblastic cell proliferation and collagen production that result in reduced bone formation and diminished mechanical properties of the newly formed bone 71-74. The effect of AGEs on osteoclast function is not completely clear. Some studies have reported significant levels of osteoclasts and increased osteoclast activity in diabetic patients 75-78, whereas other studies have reported decreased bone resorption under similar conditions 79-81.
| Long-term diabetic complication | Oral implications |
|---|---|
| Microvascular disease | · Xerostomia · Greater susceptibility of oral tissues to trauma · More opportunistic infections (e.g., candidiasis) · Greater accumulation of plaque · Greater risk of caries · Delayed wound healing · Greater susceptibility to periodontal disease |
| Peripheral neuropathy | · Oral paresthesia, including burning mouth or tongue · Altered taste sensations |
Proposed pathways of periodontitis affecting diabetes
Gingivitis and periodontitis are inflammatory conditions having a primary microbiological etiology. Gingivitis is the inflammation of gingiva with no attachment loss, whereas, in periodontitis, there is a loss of periodontal structures clinically evident as attachment loss. The host-microbial interactions lead to the production of various chemical mediators which have local and systemic effects. As both periodontal diseases and diabetes, especially type 2 diabetes, have major inflammatory components, the role of inflammatory mediators is important in the disease progression. The following mechanisms have been proposed to explain the effect of periodontal infection on diabetes mellitus,
Microorganisms involved in periodontal infection in diabetics:
As we know that the bacteria involved in periodontitis are usually anaerobic Gram-negative bacteria. They cause damage to periodontal tissues directly by releasing their virulence factors and indirectly by initiating the release of various inflammatory mediators by host immune cells 82. Gram-negative bacteria-derived lipopolysaccharide (LPS) is a potent inducer of TNF-α from monocytes and macrophages. Studies done on rat models have shown that infusion of bacterial LPS, which is a potent inducer of TNF-α, resulted in severe insulin resistance in these animals 83, 84. These findings indicate that periodontal infections may lead to insulin resistance.
The microbiological studies done on diabetic patients have not revealed ………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………
Role of pro-inflammatory factors:
As already stated, periodontal treatment has been associated with improved glycemic control and reductions in HbA1c levels 88. The reason for the improved glycemic control is the reduction in the pro-inflammatory cytokine levels locally, and therefore reduced levels of these mediators in the circulation. Two key mediators which relate periodontitis and diabetes are IL-6 and TNF-α. Both of these mediators are strong inducers of acute-phase proteins such as CRP, and both have been shown to impair intracellular insulin signaling 89, 90.
Role of TNF-α:
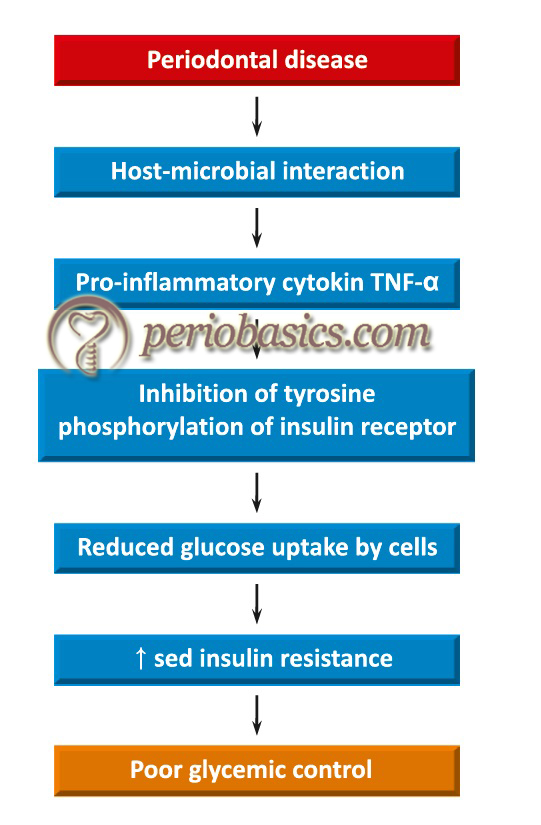
As discussed earlier, TNF-α has been found to increase insulin resistance. Under normal conditions when insulin binds to the insulin receptors on muscle and fat cells, a tyrosine residue of the cytoplasmic domain of the insulin receptor is autophosphorylated. It leads to the initiation of signal that causes glucose uptake by the cell. However, in the presence of TNF-α, this process is inhibited, thus influencing glucose uptake by the cells, resulting in insulin resistance 91-93.
TNF-α is believed to impair the tyrosine phosphorylation of insulin receptor substrate molecules, an essential step in the signal transduction pathway for insulin. This action, thereby impairs the messenger RNA (mRNA) transcription process, needed for the synthesis of insulin-responsive glucose transporter protein (GLUT-4) receptor. In addition, TNF-α causes adipocytes to release free fatty acids, which contribute to insulin resistance by impairing insulin signaling 94. A study has demonstrated that subjects with type 2 diabetes and periodontitis, who underwent periodontal treatment resulted in a significant reduction in serum levels of TNF-α that was accompanied by a significant reduction in mean HbA1c values (from 8.0 to 7.1 percent) 95.
Role of IL-6:
Elevated levels of IL-6 predict future risk of type 2 diabetes development 96-98. IL-6 induces signaling in all cells expressing the ubiquitous gp130 receptor. It is a strong inducer of C-reactive protein synthesis by hepatocytes. The role of IL-6 in insulin resistance is controversial 99. The exact mechanism of IL-6 induced insulin resistance is not clear, but recent studies have demonstrated that in the adipose tissue IL-6 mRNA are elevated in insulin-resistant humans, and the ………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Review of literature on the effect of periodontal treatment on diabetes
The effects of mediators of inflammation released during periodontitis on diabetic control have been explained well in the scientific literature. The pro-inflammatory mediators, such as TNF-α, IL-6, IL-1β and interferon gamma (IFN-γ), and increased levels of acute-phase proteins, such as C-reactive protein (CRP) have important effects on glucose and lipid metabolism. TNF-α, IL-6, and IL-1β are insulin antagonist and lipid metabolism is hampered by TNF-α. Increased CRP levels cause insulin resistance. Also, IFN-γ induces apoptosis of pancreatic β cells 103. These findings explain why periodontitis subjects have high HbA1c levels. The treatment of the periodontitis reduces the proinflammatory mediators released during host-bacterial interactions and thus, the glycemic control is improved. However, research work so far does not clearly support these findings.
Effect of non-surgical periodontal therapy on diabetes glycemic control:
Many studies have been done to evaluate the change in glycemic control in type II diabetes patients who were treated non-surgically for periodontitis. Faria-Almeida et al. (2006) 104 reported a significant improvement in the glycemic control in type II diabetes patients after non-surgical periodontal therapy. In another study, Auyeung et al. (2012) 105 reported that there was a significant improvement in the glycemic control in well-controlled diabetic patients. However, many studies have contradictory findings. Engebretson et al. (2013) 106 found that non-surgical periodontal therapy in chronic (Grade B) periodontitis patients, did not improve diabetes glycemic control. These findings were supported by a randomized controlled trial done by Gay et al. (2014) 107.
Various systematic reviews have also tried to find out the effect of non-surgical periodontal therapy in periodontitis patients on diabetic glycemic control. In a systematic review, Simpson et al. (2010) 108 reported glycemic control improvement, with an ………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………
Effect of surgical periodontal therapy on diabetes glycemic control:
There is only a little research which makes it difficult to determine the response after periodontal surgical treatment in diabetic patients. It is important to note here that surgical periodontal therapy is done on well-controlled diabetic patients and these patients usually show improved periodontal status after surgical periodontal treatment. However, in poorly controlled diabetic patients, there are more chances of recurrence of periodontal pockets. Furthermore, in these patients, the long term prognosis becomes compromised.
Conclusion
From the above discussion, we can conclude that prevention and control of periodontal disease must be considered as an integral part of diabetes control. Well-controlled diabetics have a similar incidence of periodontitis as do non-diabetics. Diabetic patients must be educated about maintenance of good oral hygiene, which can improve their periodontal health as well as glycemic control. Studies have indicated the role of AGEs and pro-inflammatory cytokines released during periodontal disease activity in increasing insulin resistance. Blocking the activity of these mediators can improve glycemic control in diabetic patients. Further investigations are required in this direction.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.