Introduction to alveolar bone
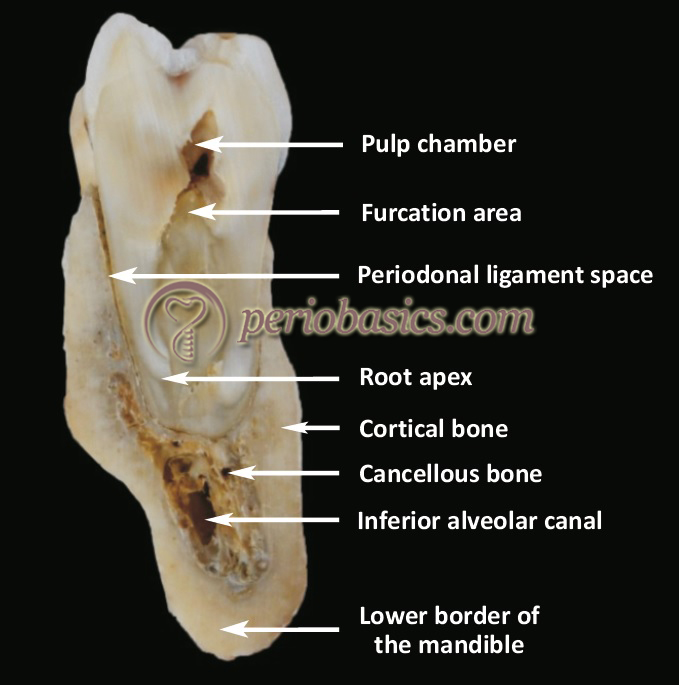
Alveolar bone is the specialized part of maxillary and mandibular bone that supports the teeth. It forms with the eruption of teeth and gradually disappears after the tooth is lost. The alveolar bone consists of an outer cortical plate which is composed of Haversian bone and compacted bone lamellae, a central spongiosa or cancellous bone and inner socket wall. The cortical plate and the bone lining the socket wall (alveolus) meet at the alveolar crest. The bone lining the socket wall is referred to as “bundle bone” because it provides attachment to principal fiber bundles of PDL. Anatomically, alveolar bone is a quite complex tissue due to its functional demands. Before discussing various aspects of alveolar bone, first we need to go through the developmental aspect and the molecular aspect of bone formation.
Basic concepts in osteogenesis
Bone is a dynamic biological tissue, composed of various metabolically active cells that are integrated into a rigid framework. The cell line involved in osteogenesis consists of preosteoblasts, osteoblasts, osteocytes and bone lining cells. These cells are of mesenchymal origin, derived from the stroma of bone marrow and from pericytes adjacent to small blood vessels in the connective tissue. Growth factors are involved in differentiation of these mesenchymal cells into osteogenic cells. These include various factors like transforming growth factor-β (TGF-β) and bone morphogenetic factor-2 (BMP-2) 396. Cell markers which indicate osteogenic differentiation are osteocalcin, osteonectin, alkaline phosphatase and bone sialoprotein. The cells responsible for bone resorption are osteoclasts. Let us now try to understand how the bone forms.
Know More…
Periosteum:
It is a well-vascularized fibrous sheath which covers the external surface of most bones except the articular surfaces, areas of tendon insertions, or sesamoid bone surfaces. Periosteum contains osteogenic cells that regulate the outer shape of bone and work in coordination with inner cortical ‘endosteum’ (tissue lining the internal bone cavities) to regulate cortical thickness and size. Periosteum consists of an outer fibrous layer and an inner cellular layer (cambium). The outer fibrous layer can be subdivided into two parts: The superficial portion and deep portion. The superficial portion is composed of a predominant collagenous matrix and few elastic fibers. It is generally inelastic and is relatively poor in the cell population. This layer is highly vascularized and provides nutrient supply to the underlying bone. It is also rich in nerve endings. The deep portion of the outer fibrous layer is fibroelastic since it contains many elastic fibers and so has significant elasticity. This layer also contains abundant collagen fibers, but is less vascularized as compared to the superficial layer.
The inner cambium layer is highly cellular. It is composed of mesenchymal progenitor cells, differentiated osteogenic progenitor cells, osteoblasts, fibroblasts 397, microvessels 398, and sympathetic nerves 399. This layer is directly placed in contact with the bone and is formed of three to four cell lines. Osteoblasts are in direct contact with the bone surface. The cambium is thickest in the fetus and becomes progressively thinner with age. In adults, the cambium layer is so thin that it cannot be distinguished from the covering fibrous layer 400.
Bone formation
Bone formation occurs by two mechanisms: intramembranous bone formation and endochondral bone formation. The intramembranous bone formation occurs by the inner periosteal osteogenic layer with bone synthesized initially without the mediation of a cartilage phase. On the other hand, endochondral bone formation occurs on a mineralized cartilage scaffold. The flat bones of the skull, maxilla and mandible are formed by intramembranous ossification. The main steps involved in intramembranous ossification are: formation of ossification center, calcification, formation of trabeculae and development of the periosteum. The mesenchymal stem cells are the primary cells involved in the initiation of bone formation. These cells differentiate into osteoblasts, which deposit osteoid at the site of bone formation. During endochondral ossification, bone formation is initiated with the development of cartilaginous model followed by its growth. After this, the primary ossification center is formed where the process of ossification is initiated. Then secondary ossification center/centers are formed which give rise to the final shape of the bone.
Matrix orientation
Alveolar bone is basically composed of three types of bones: woven bone, cortical bone, and cancellous bone. The woven bone is immature bone, which is formed primarily during embryonic development, during fracture healing and in some pathological states such as hyperparathyroidism and Paget’s disease 401. The cortical bone (also known as compact or lamellar bone) is formed by the maturation of woven bone. It has a well organized vascular structure. The primary structural unit of cortical bone is an osteon. An osteon consists of a cylindrical-shaped lamellar bone that surrounds longitudinally-oriented vascular channels known as ‘Haversian canals’ and horizontally oriented canals known as ‘Volkmann canals’. The Volkmann canals connect the adjacent osteons, thus making a well organized three dimensional structure. The third type of bone or the cancellous bone (also known as trabecular bone) has a honeycomb-like structure with hematopoietic tissue filling the spaces within the bone. The trabeculae of the cancellous bone are mostly oriented perpendicular to external forces to provide structural support 402, 403.
Development of alveolar bone
As already stated, the alveolar processes of maxilla and mandible develop alongside with the eruption of teeth. During the second month of fetal life, there is the formation of a groove in maxilla and mandible that open towards the surface of the oral cavity, enclosing the developing tooth buds. The formation of alveolar bone starts with the formation of tooth-supporting apparatus. A major portion of the alveolar process begins to form with root formation and eruption of the teeth. The developing tooth buds in the maxilla and mandible are surrounded by loose woven bone spicules. With the development of the teeth, the trabeculae of the alveolar bone are formed. As permanent teeth develop, they start resorbing the roots of deciduous teeth which are ultimately shed. Finally, the permanent teeth occupy the alveolar sockets. The alveolar bone is formed around the teeth by intramembranous ossification.
Various parts of alveolar bone
The alveolar bone is made up of two distinguishable parts, alveolar bone proper and supporting alveolar bone. The alveolar bone proper is made up of thin lamellae of bone (cortical bone) which surrounds the root. When seen on a radiograph, the alveolar bone proper appears as radiopaque line known as “lamina dura”. The principal collagen fibers (Sharpey’s fibers) from the PDL are inserted into this bone. Because of insertion of these fibers, alveolar bone proper is also known as “bundle bone”. The alveolar bone proper is perforated by many openings providing passage to the blood vessels, lymphatics, and nerves. Therefore, this bone is also known as “cribriform plate”.

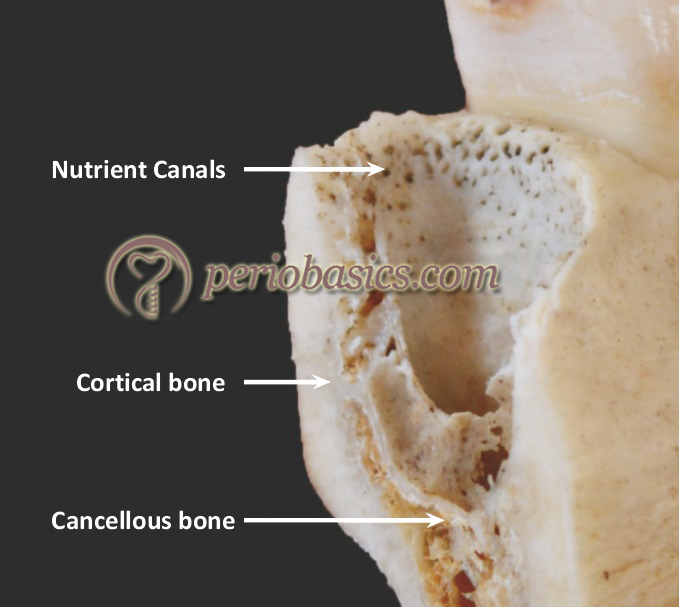
The supporting alveolar bone is the remaining bone of alveolar process except alveolar bone proper. This bone consists of cortical bone and spongy bone. The cortical bone provides the outer covering to the alveolar process. It is lamellated and is covered by the periosteum. The inner and the outer cortical plates meet at the alveolar crest. The thickness of the cortical plates in the posterior areas is usually about 1.5 to 3 mm. In anterior teeth, the thickness of cortical plates is highly variable. The cortical bone is thicker in the mandible than in the maxilla. The spongy bone is present between the outer and inner cortical plates. The trabeculae of spongy bone are arranged in two patterns,
Type I: In this type, the trabeculae are arranged in a ladderlike fashion. This type of arrangement is more commonly seen in the mandible.
Type II: Here, the trabeculae are arranged in an irregular manner. These are more commonly seen in the maxilla.
Alveolar bone crest:
The alveolar bone crest more or less parallels the CEJ of the teeth, located 1-3 mm apical to it. This distance increases with age 404. The shape of the alveolar crest depends on many factors, including the contour of the CEJ, degree of tooth eruption and alignment of teeth. Similarly, the shape of the interdental bone crest depends on factors like the contour of the enamel, width of interdental space, the state of eruption and position of teeth in the arch. The contour of the alveolar bone margin is usually scalloped as described for gingiva, but it is not always the case. The contour of the crest of the bone margins depends on the shape of the roots and the thickness of the cortical plates. When the root is flat, the contour of the alveolar bone margin is also flat or straight. More curved is the root surface; more scalloped is the marginal bone. A thin bone covering the tooth roots is more scalloped as compared to thick bone which is more flattened.
The shape of interdental septum depends on ………. Content available in the hard copy of the website……….. Content available in the hard copy of the website………………. Content available in the hard copy of the website……….
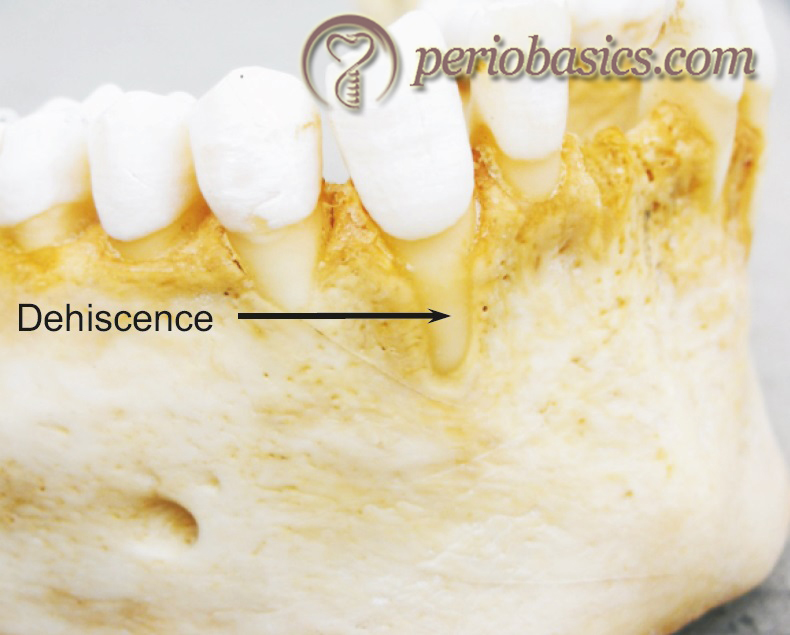
Dehiscence and fenestrations
Dehiscence and fenestrations are commonly found in the alveolar bone. A dehiscence is the loss of alveolar bone on the facial (rarely lingual) aspect of a tooth that leaves a characteristic oval, root-exposed defect from the CEJ apically. A fenestration is a circumscribed hole in the cortical plate over the root surface which does not communicate with the crestal margin. In other words, we can say that unlike dehiscence, fenestration is bordered by alveolar bone along its coronal aspect.

Composition of alveolar bone
Like any other bone, alveolar bone is composed of around 65% of inorganic and 35% of organic proportions. Principal inorganic ions present in bone are calcium and phosphate. Other minerals present are carbonates, citrates and a trace amount of other ions including sodium, magnesium, and fluorine. The inorganic content is primarily made up of hydroxyapatite constituting around 65-70% of the bone structure. More than 90% of the organic bone matrix is made up of collagenous proteins, primarily collagen Type I with a minor component of collagen Type V. The remaining portion of the bone matrix is formed of non-collagenous proteins, including hyaluronan, proteoglycans, GAGs (chondroitin sulfate, keratan sulfate) multi adhesive glycoproteins (osteonectin, sialoproteins I and II, Osteopontin), osteocalcin, growth factors and cytokines.
Cellular components of alveolar bone
Osteoblasts:
These are the bone forming cells, which express parathyroid hormone (PTH) receptors and have several important roles in bone remodeling including expression of osteoclastogenic factors, production of bone matrix proteins, and bone mineralization 405. Osteoblasts are derived from pluripotent mesenchymal stem cells and their differentiation is controlled by the master transcription factor RUNX2 (runt-related transcription factor 2); also known as CBFA1 (core-binding factor A1) 406, 407. During differentiation, osteoblasts express a specific cadherin referred to as OB-cadherin 408. Osteoblasts secrete collagenous and non-collagenous matrix components of the bone matrix. They also secrete matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs). Many regulatory components such as cytokines and growth factors are also secreted by these cells. Because these are actively synthesizing cells, they contain abundant endoplasmic reticulum and Golgi complexes.
During routine hematoxylin-eosin staining, these cells demonstrate intense basophilic cytoplasm. Mature osteoblasts, which are actively depositing bone matrix have a cuboidal or columnar shape. Osteoblasts attach to the underlying bone via plasma membrane integrins, including α5β1, αvβ3, α3β1, α6β1 and α1β1 integrins located on the plasma membrane attachment plaques 409. These integrins bind to collagen and/or fibronectin in the bone, which is an essential step during bone formation. The expression of integrins on osteoblast cell membrane is downregulated by ……Content available in the hard copy of the website……….. Content available in the hard copy of the website………………. Content available in the hard copy of the website………
Osteocytes:
These are osteoblasts that get entrapped into the bone lacunae during bone deposition. These cells comprise more than 90% of bone cells within the matrix or on bone surfaces 411. Osteocytic lacunae are connected by canaliculi containing their cytoplasmic processes. These canaliculi serve as pathway to supply nutrients and oxygen from blood capillary to osteocytes. The main function of these cells is, control of the extracellular concentration of calcium and phosphorus, as well as in adaptive remodeling behavior via cell-to-cell interactions in response to the local environment. Research has demonstrated that osteocytes can send signals of bone resorption to osteoclasts during bone remodeling 412. They are able to resorb bone on the lacunar walls and are also able to deposit new bone. The process of bone resorption by osteocytes is also known as “osteocytic osteolysis” 413.
Osteoclasts:
These are the bone resorbing cells. Osteoclasts are multinucleated cells, which are controlled by various hormonal and cellular mechanisms. Macrophage-colony stimulating factor (M-CSF) is a critical factor for osteoclast differentiation along with a RANK / RANKL system which is responsible for osteoclast differentiation and maturation 414. Molecules like prostaglandin E2 (PGE2), interleukin (IL)-1, 1,25-(OH)2D3, parathyroid hormone (PTH) and PTH-related protein upregulate the expression of RANKL in osteoblast lineage cells, thereby stimulating osteoclastogenesis. On the other hand, OPG, which works as a decoy receptor for RANKL inhibits osteoclastogenesis. Calcitonin, which is a hormone, also inactivates osteoclasts.
During osteoclast action, the plasma membrane in the area facing the bone matrix becomes folded (ruffled). This ruffled border is closely associated with bone resorption. Bone resorption is achieved by dissolution of mineral components consisting of hydroxyapatite and degradation of organic contents of bone matrix. The carbonic anhydrase (which converts CO2 and H2O into H+ and HCO3) and vacuolar-type H+-ATPase in ruffled border membrane result in the formation of shallow erosive pits on the bone surface called “Howship lacunae” 415. The chloride channel (CIC)-7 play an important role in the maintenance of cytoplasmic ion balance. The organic content of the bone matrix is degraded by lysosomal enzymes such as cathepsin K 416, 417 and MMP-9 418.
Bone lining cells:
Bone lining cells cover inactive (non-remodeling) bone surfaces. These cells have a flattened shape and contain a few cell organelles. The intracellular characteristics of bone lining cells suggest that bone lining cells are hardly engaged in bone formation. Various terminologies have been used in the past to describe these cells, including surface osteocytes, inactive osteoblasts, endosteal lining cells and flattened mesenchymal cells. These cells are thought to be quiescent osteoblasts and are found in close proximity to each other, joined by adherens junctions. An extensive canalicular network connects the osteoblasts, osteocytes, and bone lining cells. The primary function of the osteocyte-osteoblast/lining cell syncytium is mechanosensation 424.
Functions of alveolar bone
The primary function of alveolar bone is to hold the teeth firmly in position and to transfer the occlusal forces to the basal bone. It is a dynamic tissue and adapts to withstand the occlusal forces put on the teeth. It provides vascular supply to PDL and cementum. It houses and protects the permanent teeth while supporting the deciduous teeth.
Remodeling and repair of alveolar bone
The alveolar bone is subjected to continuous remodeling to compensate for its functional demands. Initially, there is deposition of immature or woven bone. This bone is gradually replaced by mature or lamellar bone. The process of maturation is intimately related to the vascular bed. During lamellar bone formation, there is radial bone deposition around the central connective tissue core containing blood vessels and nerves. The density of bone minerals increases with time in an osteon to reach the peak level of mineralization. Throughout the lifetime of an individual, there is a physiologic migration of teeth in the mesial direction towards the midline, also known as “physiologic mesial drift”. To allow this mesial migration, the alveolar socket wall is resorbed on the mesial surfaces of the root and new bone is deposited on the distal surfaces of the socket wall. The bone resorption may be the result of mild PDL compression on the mesial root surfaces. On the other hand stretching of PDL on the distal surfaces of the roots may result in bone deposition.
The PDL collagen fiber bundles get embedded into this new bone, which is referred to as “bundle bone”. The new bone is deposited on the older bone within a short duration of time. A “reversal line” separates the …….Content available in the hard copy of the website……….. Content available in the hard copy of the website………………. Content available in the hard copy of the website……..
Any fracture in the alveolar bone heals like any other bony fracture in the body. Within a few hours following fracture, the osteoprogenitor cells from the periosteum, endosteum and from bone marrow divide and migrate towards the site of injury. The blood clot which is formed between the fractured bone serves as a framework for cell migration and is rapidly populated by the immature osteogenic cells. The cells in the clot, including platelets and other cells derived from blood act as a source of various growth factors including bone morphogenetic proteins (BMPs), fibroblast growth factors (FGF), platelet-derived growth factor (PDGF) and insulinlike growth factors (IGFs), which are responsible for the stimulation of the cascade that leads to bone formation. New blood vessels are formed which penetrate the clot within next 24 hours. Within a few days, callus is formed between the fractured fragments of the bone. Callus is composed of immature woven bone, which is gradually remodeled to form mature bone.
Turnover of alveolar bone
The turnover rate of alveolar bone is more than the other parts of the skeleton. The highest rate of remodeling is that of the cribriform plate, bone adjacent to PDL. The turnover rate of alveolar bone is particularly high during tooth eruption. During tooth eruption, there is rapid bone remodeling around the tooth till it reaches its final position in occlusion.
Conclusion
Alveolar bone surrounds and supports the teeth and is a very important component of the periodontal apparatus. The loss of alveolar bone is the hallmark of periodontitis. Clinically it can be detected by loss of attachment or apical migration of alveolar crest in radiographs. A detailed description of pathophysiology of alveolar bone loss is available in “Pattens of bone destruction in periodontal diseases”.
References
References are available in the hard copy of the website.