Introduction
The periodontium, a complex and highly specialized system of tissues, is designed to anchor the tooth within the alveolar bone and withstand the myriad forces of mastication, parafunction, and even speech. For decades, the relationship between occlusion and the health of this supporting apparatus has been a source of intense clinical scrutiny and academic debate. The central, often contentious, question has been: does an “occlusal abnormality” cause periodontal disease? The answer, now supported by a robust body of evidence, is nuanced. Occlusal forces are not initiators of inflammatory periodontal disease. The primary etiological agent for periodontitis remains the microbial biofilm (dental plaque). However, the role of occlusion shifts from being an initiator to a powerful modulator of the disease’s progression and the effectiveness of its treatment.
This paradigm positions occlusal forces as a critical co-factor. When the periodontium is healthy, with a full, uninflamed attachment apparatus, it possesses a remarkable adaptive capacity. It can remodel, via the periodontal ligament (PDL), to accommodate significant occlusal stresses. This is the state of physiological adaptation. Conversely, when inflammation, driven by bacterial plaque, weakens the periodontal tissues, reducing the bone support and the structural integrity of the PDL, the same occlusal forces can become traumatic. This results in pathological changes, a condition termed “trauma from occlusion.” The interplay creates a vicious cycle: inflammation reduces the tissue’s tolerance to force, and excessive force can exacerbate the inflammation, leading to accelerated attachment loss, increased tooth mobility, and compromised healing outcomes.
Therefore, the contemporary practice of periodontics cannot afford to view occlusion as an afterthought. A comprehensive periodontal assessment must include a meticulous occlusal evaluation. The goal is not to create a “perfect,” idealized occlusion but to establish a functional, stable, and atraumatic occlusal environment that is compatible with the long-term health and stability of the periodontium.
What is Occlusion and Its Types
Occlusion, in its broadest dental definition, refers to the static and dynamic contact relationships between the maxillary and mandibular teeth. It is a complex, multifaceted concept that encompasses not only how teeth fit together but also the functional and parafunctional movements of the mandible, the neuromuscular system that controls them, and the adaptive capacity of the supporting structures. Understanding its various classifications is fundamental to assessing its impact on periodontal health.
Occlusion can be categorized in several ways. Static occlusion refers to the contact of teeth when the mandible is in a fixed, closed position. The most clinically relevant static position is centric relation (CR) , a reproducible, musculo-skeletally stable position of the condyles in the fossae, independent of tooth contact, and maximum intercuspation (MI) , also known as centric occlusion (CO), which is the position of maximum interdigitation of teeth, guided by the occlusal surfaces. A key clinical goal is often to achieve harmony between CR and MI, where the mandible closes in CR with even, simultaneous tooth contacts, or with a very slight, controlled slide into MI.
Dynamic occlusion describes the contact relationships during mandibular movements. This includes:
-
Lateral excursion: Contact patterns on the working (laterotrusive) and non-working (mediotrusive) sides. Concepts such as canine guidance (where the canine is the sole tooth contacting during lateral movement, discluding all posterior teeth) or group function (where multiple teeth on the working side share the load) are defined here. Non-working side contacts, once believed to be highly destructive, are now understood to be less pathological than previously thought but still require evaluation.
-
Protrusive excursion: Contacts that occur as the mandible moves forward. The anterior teeth typically provide guidance, discluding the posterior teeth.
From a periodontal perspective, a more clinically relevant classification focuses on the nature and consequence of occlusal forces. This distinguishes between:
-
Physiological Occlusion: This is a state of harmony where occlusal forces are within the adaptive capacity of a healthy periodontium. There may be wear facets, minor tooth mobility, and occlusal contacts that are stable over time. There is no associated pain, progressive pathology, or signs of traumatic injury to the periodontium. The periodontium remodels to accommodate the forces.
-
Trauma from Occlusion (TFO): This is defined as injury to the periodontium (or the pulp) resulting from excessive occlusal forces. It is a key concept in periodontics and is further sub-classified:
-
Acute TFO: Results from a sudden, impactful force, such as biting on a hard object (e.g., an olive pit) or a restoration that is inadvertently left high. The clinical signs are pain on biting, tenderness to percussion, and possibly increased mobility.
-
Chronic TFO: A more insidious condition resulting from gradual changes in occlusal contacts due to tooth wear, drifting, extrusion, or parafunctional habits like bruxism or clenching over a long period.
TFO is also classified based on the presence of inflammation: -
Primary TFO: Occurs when excessive occlusal forces are applied to a periodontium with normal height and health. The tissues are healthy, but the forces exceed their adaptive capacity.
-
Secondary TFO: Occurs when normal or excessive occlusal forces are applied to a periodontium that has been weakened by inflammatory bone loss (periodontitis). This is the most common clinical scenario and the one of greatest concern in periodontics, as the reduced attachment apparatus is far more susceptible to injury.
-
-
Non-functional Occlusion (Parafunction): This encompasses activities such as bruxism (grinding) and clenching that are not part of normal functions like chewing or swallowing. These habits generate sustained, high-magnitude forces, often for prolonged periods, and are a primary source of occlusal pathology, including attrition, fractures, and TFO.
Historical Aspect of Occlusal Research in Periodontics
The journey to understanding the relationship between occlusion and periodontal disease is a fascinating historical arc, moving from a dogmatic causal belief to a sophisticated, evidence-based understanding of force as a co-factor. In the late 19th and early 20th centuries, the prevailing dental philosophy was one of mechanical determinism. Pioneering figures like J. Sim Wallace and Alfred Paulsen proposed that improper occlusion was the primary cause of periodontal disease. This “traumatic occlusion” theory was further championed by Edward H. Angle, the “father of modern orthodontics,” who viewed occlusion as the cornerstone of dental health. The logic was seemingly intuitive: if teeth were not properly aligned, the “stress” from malocclusion would lead to inflammation, bone loss, and eventual tooth loss.
This philosophy reached its zenith in the mid-20th century with the work of B.B. McCall and Samuel Charles Miller, who advocated for aggressive occlusal adjustment (coronoplasty) as a primary treatment for periodontal disease, often without consideration of the microbial etiology. The idea was to “balance the bite” to eliminate “occlusal traumatism,” which was believed to be a direct cause of periodontitis. This era was characterized by the widespread use of articulators and elaborate gnathological systems aimed at creating a “theoretically perfect” occlusion, often involving extensive and irreversible tooth modification.
A critical shift in this paradigm began with the groundbreaking work of Dr. Helmut Zander and his colleagues at the Eastman Dental Center in the 1950s and 1960s. Their seminal animal studies, using squirrel monkeys and dogs, began to systematically separate the effects of inflammation from the effects of occlusal trauma. They demonstrated, unequivocally, that occlusal forces alone, in the absence of plaque-induced inflammation, did not cause progressive periodontitis. They could induce bone loss and mobility, which they termed “trauma from occlusion,” but crucially, these changes were reversible once the force was removed. Conversely, plaque-induced inflammation, without occlusal trauma, resulted in the classic features of periodontitis: pocket formation, irreversible bone loss, and attachment loss. This was a monumental step in refuting the long-held belief that occlusion was a primary etiological agent.
Simultaneously, the Scandinavian school of periodontics, led by Jens Waerhaug, introduced a different perspective. Using meticulous histology, Waerhaug observed that the pattern of bone loss in periodontitis consistently followed the apical migration of the subgingival biofilm. He argued that the inflammatory front was the key determinant of the level of the connective tissue attachment and bone. He posited that if occlusal forces were truly destructive, they would create predictable patterns of bone loss (e.g., angular defects, furcation involvement) that were independent of the plaque front. His conclusion was that the primary, non-negotiable driver of attachment loss was inflammation, and that the role of occlusion was secondary—primarily manifesting as increased tooth mobility, but not as a direct cause of pocket formation.
The work of Sigurd P. Ramfjord, another towering figure in periodontology, further refined this understanding. His longitudinal studies, including the landmark Michigan study, provided clinical evidence that occlusal adjustment did not significantly alter the long-term progression of periodontitis when compared to meticulous plaque control alone. This did not mean occlusion was irrelevant, but rather that its management was not a substitute for effective infection control. Ramfjord and his contemporaries helped establish the modern concept of occlusion as a co-destructive factor. This concept acknowledged that while inflammation was the primary driver of tissue destruction, the presence of TFO could modify the pathway of that destruction (e.g., creating angular versus horizontal bone loss), accelerate its progression, and create a more challenging environment for periodontal healing and long-term stability. The historical narrative, therefore, transitioned from viewing occlusion as the cause to viewing it as a modulator of periodontal disease, a perspective that forms the bedrock of contemporary clinical practice.
Animal and Human Studies
The evolution of our understanding of the occlusion-periodontium interface is built upon a foundation of meticulously designed animal experiments and longitudinal human clinical trials. These studies have served to dissect the complex interplay between microbial inflammation and mechanical force.
Animal Studies
Animal models, particularly in non-human primates and dogs, have been invaluable because they allow for the controlled introduction of plaque and occlusal forces, which is ethically and practically impossible in human studies.
-
The Eastman Dental Center Studies (Zander, Glickman, et al.): This series of experiments in the 1950s-70s was pivotal. A classic study by Waerhaug (1955) and later by Glickman and Smulow (1965) used squirrel monkeys. They created experimental periodontitis by placing wire ligatures around teeth to accumulate plaque. In separate quadrants, they induced occlusal trauma by creating high restorations or grinding facets to alter occlusal contacts. The key findings were:
-
Glickman & Smulow, 1965: “Effect of occlusal trauma on the periodontium of the squirrel monkey.” Journal of Periodontology. They found that occlusal trauma alone (in the absence of plaque) caused widening of the PDL, angular bone loss, and increased mobility, but this was reversible upon removal of the trauma. Plaque-induced inflammation alone caused progressive, irreversible horizontal bone loss. Critically, when both factors were combined, the destruction was more severe, and the bone loss took on an angular, infrabony pattern that was characteristic of the combined insult. This was the first strong evidence for the concept of “co-destruction.”
-
Lindhe & Svanberg, 1974: “Influence of trauma from occlusion on progression of experimental periodontitis in the beagle dog.” Journal of Clinical Periodontology. This landmark study further refined the concept. They created experimental perioditis in dogs and then induced jiggling-type trauma (alternating occlusal forces) on specific teeth. Their results showed that while TFO alone did not cause attachment loss, it significantly accelerated the rate of attachment loss and bone loss in teeth with pre-existing periodontitis. This reinforced the idea that a compromised periodontium is more vulnerable to the effects of occlusal forces.
-
-
Studies on Jiggling Forces: Subsequent animal studies focused on the nature of the force. It was demonstrated that jiggling forces (alternating horizontal forces) were far more destructive to a periodontium already compromised by inflammation than static or unidirectional forces. This is because jiggling forces prevent the PDL from adapting and continuously compress and stretch the tissues, disrupting the microcirculation and impeding repair.
Human Studies
Human studies, while less invasive, have provided crucial clinical evidence regarding the impact of occlusal management on periodontal treatment outcomes.
-
The Michigan Longitudinal Study (Ramfjord et al.): This was a landmark 15-year study that followed patients with periodontitis who received comprehensive treatment.
-
Ramfjord, et al., 1975: “Subgingival curettage versus surgical periodontal therapy.” Journal of Periodontology. In subsequent analyses, they specifically examined the role of occlusal adjustment. They concluded that while occlusal adjustment could reduce tooth mobility, it did not have a significant, measurable effect on long-term attachment levels or tooth loss in patients who maintained excellent plaque control. This study was highly influential in de-emphasizing occlusal adjustment as a primary treatment and reinforcing the supremacy of plaque control and inflammation management.
-
-
Studies on Tooth Mobility and Treatment Outcomes: Several human studies have investigated the effect of treating TFO on the outcomes of periodontal therapy.
-
Fleszar, et al., 1980: “The effect of occlusal adjustment on the periodontal status of teeth with exaggerated mobility.” Journal of Periodontology. This study showed that in patients with chronic periodontitis, teeth that received occlusal adjustment in addition to scaling and root planing showed a greater reduction in mobility and a more favorable healing response than those that did not receive adjustment. This suggested that in specific cases—particularly those with significant mobility—managing TFO could enhance the results of non-surgical therapy.
-
Harrel & Nunn, 2001: “The effect of occlusal therapy on the progression of periodontitis.” Journal of the American Dental Association. This more recent study provided compelling evidence. They compared the progression of periodontitis in patients who received occlusal therapy (adjustment, splinting) as part of their treatment versus those who did not. They found that patients who did not receive occlusal therapy were significantly more likely to have disease progression (≥ 2 mm attachment loss) over a 5-year period. This study, along with others, revitalized the importance of occlusal management, suggesting that while it may not be essential in all cases, it is a critical component for long-term stability in susceptible patients.
-
-
Bruxism and Implant Studies: Human studies on dental implants have provided an indirect but powerful insight into the role of occlusal forces. Implants lack a PDL and therefore have no physiological feedback mechanism to dampen forces.
-
Studies have consistently shown that parafunctional habits (bruxism) are a major risk factor for implant complications, including technical failures (screw loosening, fracture) and marginal bone loss. This underscores that in a system with a reduced or absent adaptive capacity, occlusal force management becomes paramount. Greenstein, et al., 2016: “The role of occlusion in implant failure: A review.” Compendium of Continuing Education in Dentistry. This review synthesized evidence showing that uncontrolled occlusal forces are a primary cause of late implant failure and prosthetic complications.
-
In summary, the collective evidence from animal and human studies establishes a clear hierarchy. Inflammation is the sine qua non for periodontitis. However, occlusal forces, particularly when excessive, parafunctional, or jiggling, act as a potent co-factor that can:
-
Alter the pattern of bone loss (from horizontal to angular).
-
Accelerate the rate of attachment loss in the presence of inflammation.
-
Compromise the healing response to periodontal therapy.
-
Increase the risk of failure for complex restorative and implant treatments.
Glickman and Waerhaug’s Concept
The mid-20th century was a crucible for ideas regarding the occlusion-periodontitis relationship, and no two perspectives were more influential, or seemingly more contradictory, than those of Irving Glickman and Jens Waerhaug. Their conceptual frameworks, while appearing to be at odds, ultimately provided the intellectual synthesis that defines our modern understanding.
Irving Glickman’s Theory: The Co-Destructive Factor
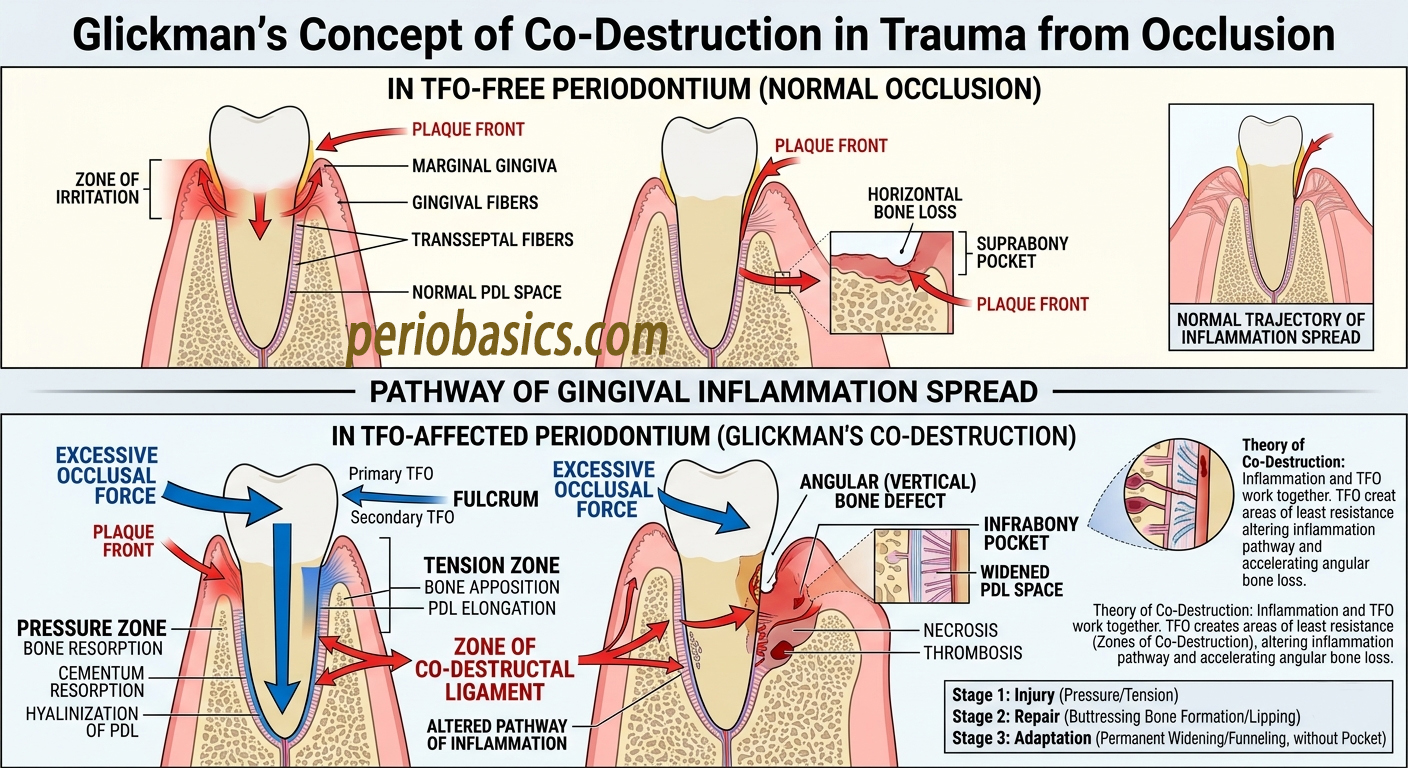
Glickman, based heavily on his seminal animal research at Tufts University, proposed a model that elegantly explained how occlusion and inflammation could interact. He did not view occlusion as a primary cause of periodontitis but as a potent modifier of its progression. His core concept was that trauma from occlusion (TFO) and inflammation are co-destructive factors. Their interaction, according to Glickman, determined the nature and severity of periodontal destruction.
He described two distinct pathways for this interaction:
-
Zone of Irritation: This concept described a scenario where the primary driver of destruction is inflammation. Glickman proposed that occlusal trauma could funnel or “channel” the inflammatory infiltrate from the gingival margin into the deeper structures of the periodontium. The trauma, by causing microfractures, vascular changes, and altering the PDL fiber architecture, created a pathway of least resistance. The plaque-induced inflammation, instead of spreading horizontally along the bone crest, would travel apically along these traumatized pathways, leading to the formation of angular (infrabony) defects. In this model, TFO does not cause the bone loss itself but dictates its morphology. This explained the clinical observation that patients with similar levels of plaque could have very different patterns of bone loss—some generalized and horizontal, others localized and angular.
-
Zone of Necrosis: This concept described a more direct and destructive interaction. Glickman hypothesized that in areas where both inflammation and TFO were simultaneously present, there was a synergistic effect. The combined insult of microbial toxins and excessive mechanical pressure would overwhelm the tissue’s repair capacity, leading to necrosis and an accelerated rate of attachment loss. This was supported by his animal studies, where teeth subjected to both ligature-induced periodontitis and occlusal trauma exhibited more rapid and severe destruction than those with either factor alone.
Glickman’s clinical implications were profound. He argued that the presence of TFO could convert a manageable, horizontal pattern of bone loss into a more complex, angular pattern that was difficult to treat and prone to recurrence. Therefore, he advocated for occlusal adjustment not as a treatment for periodontitis per se, but as a necessary step to eliminate the co-destructive factor, thereby allowing the primary therapy (plaque control and inflammation resolution) to be more effective. He believed that for healing to occur and stability to be achieved, the occlusal environment had to be rendered non-traumatic, especially after surgical procedures.
Jens Waerhaug’s Theory: The Plaque-Front Concept
In contrast, Jens Waerhaug, working at the University of Oslo, offered a perspective based on meticulous histometric analysis of human autopsy material. His central tenet was that the plaque front—the apical extension of the subgingival biofilm—was the sole determinant of the level of connective tissue attachment and the crest of the alveolar bone.
Waerhaug’s methodology was to measure, with extreme precision, the distance from the plaque front to the apical extent of the junctional epithelium and the crest of the bone. His key findings, published in a series of papers in the 1950s and 1960s, included:
-
There was a consistent, predictable distance (approximately 0.5-1.5 mm) between the plaque front and the bone crest, which he termed the “biological width.”
-
In cases of periodontitis, the bone resorption consistently followed the apical migration of the plaque. The bone was never found apical to the plaque front.
-
He examined cases that had been clinically diagnosed with “trauma from occlusion,” including teeth with angular defects and furcation involvements. In every instance, he found that the bone loss did not extend beyond the plaque front. The angular defect was not caused by the occlusal force per se, but rather the plaque had advanced further along the root surface on one aspect of the tooth than another, and the bone simply followed.
Waerhaug’s conclusion was unequivocal: occlusal trauma does not cause pocket formation or bone loss. He argued that the forces of occlusion could not “rip” the periodontal fibers from the tooth. The destruction was always mediated by the inflammatory process. He acknowledged that occlusal forces could cause tooth mobility, PDL widening, and even bone resorption (as seen in primary TFO), but he differentiated this from the irreversible, progressive attachment loss of periodontitis. He viewed mobility as a clinical sign, not a cause, of disease progression. He famously stated that the primary goal of periodontal therapy was the elimination of the plaque front, and that once this was achieved, the periodontium could usually adapt to the existing occlusal forces.
Synthesis and Reconciliation
For decades, the field was polarized between these two viewpoints. However, the modern perspective reconciles Glickman and Waerhaug by acknowledging that they were describing different, yet complementary, aspects of the same disease process.
-
Waerhaug was correct about the initiation and primary progression of attachment loss. The subgingival biofilm is the sine qua non for periodontitis. Without it, TFO does not cause irreversible periodontitis. His histometric evidence is irrefutable: the bone level follows the plaque front.
-
Glickman was correct about the modulation of the pathway and rate of destruction. In the presence of inflammation, TFO can redirect the inflammatory spread, leading to angular defects. It can also accelerate the rate at which attachment is lost, as demonstrated in the Lindhe and Svanberg dog studies.
The combined model is therefore a synergistic one. Plaque provides the potential for destruction. Occlusal trauma determines, to a large extent, the pattern (angular vs. horizontal) and rate of that destruction. A patient with a heavily inflamed periodontium and no TFO may experience slow, generalized horizontal bone loss. A patient with a similar level of inflammation but with significant parafunction and occlusal discrepancies may develop rapidly progressive, localized angular defects, leading to premature tooth loss.
This synthesis forms the basis for contemporary clinical management: the primary, non-negotiable treatment is the control of inflammation (plaque). However, once inflammation is controlled, the clinician must then evaluate the residual occlusal environment. If the forces are deemed excessive in relation to the reduced periodontium, or if they are compromising the stability of the dentition, then occlusal therapy—including adjustment, splinting, or reconstruction—is indicated to create a stable, long-term environment. The legacy of Glickman and Waerhaug is a more nuanced, evidence-based approach that recognizes the distinct but interacting roles of these two critical factors.
How to Identify Occlusal Abnormalities
Identifying occlusal abnormalities in a periodontal patient requires a systematic, multi-faceted approach that integrates clinical history, visual inspection, functional analysis, and mobility assessment. The goal is not just to describe occlusal contacts, but to determine if the existing forces are within the adaptive capacity of the patient’s periodontium.
The process begins with a patient history, which is often the most revealing. Key questions include:
-
Parafunction: Does the patient wake up with jaw soreness, headaches, or muscle fatigue? Do they have a history of clenching or grinding, often reported by a sleep partner? These point to bruxism, a major source of high-magnitude, chronic forces.
-
Symptoms: Is there any pain or discomfort on biting? Are there teeth that feel “high” or “loose”? Has the patient noticed any recent changes in tooth position, such as flaring, spacing, or extrusion?
-
Restorative History: Have there been recent dental procedures (crowns, fillings) that have altered the bite? A recent “high” restoration is a classic cause of acute TFO.
The clinical examination follows, focusing on both the teeth and the periodontium.
-
Mobility: Tooth mobility is a cardinal sign of occlusal force exceeding the support. It should be graded using a standardized system (e.g., Miller’s Index: Grade I—slight movement <1mm horizontally; Grade II—moderate movement >1mm horizontally; Grade III—severe horizontal and vertical movement). However, it’s crucial to remember that mobility can also result from inflammation alone (inflammatory mobility). The key is to assess mobility after initial inflammation has been controlled, as residual mobility is more likely to be trauma-induced.
-
Fremitus: This is a palpable vibration felt on the tooth or crown when the patient taps or grinds in various excursive movements. It indicates that the tooth is receiving excessive occlusal load and is a more sensitive indicator of TFO than mobility in its early stages. Fremitus is typically assessed by placing a finger on the facial aspect of the tooth and asking the patient to clench or move their jaw.
-
Wear Facets: The presence, location, and severity of occlusal wear (attrition) are indicators of parafunction. Wear that is not age-appropriate, or that is characterized by polished, shiny facets, especially on non-functional cusps (e.g., maxillary palatal cusps, mandibular buccal cusps), is highly suggestive of bruxism.
-
Occlusal Contacts: The pattern of occlusal contacts in centric occlusion (MI) and in excursive movements (protrusive, laterotrusive) must be evaluated. This is best done using articulating paper of different thicknesses and colors (e.g., thin blue for MI, thick red for eccentric movements). The number, location, and intensity of these contacts are recorded. A key abnormality is occlusal discrepancies, such as a single, premature contact that causes a “deflective” slide into MI, or balancing side (non-working) interferences that were historically, but not universally, considered destructive.
-
Other Signs: Tooth migration (diastema formation, flaring) or extrusion (the tooth appears longer) can indicate a loss of proximal and occlusal stability. Furcation involvement can be both a result of and a complicating factor for TFO. Muscle palpation of the masticatory muscles (masseter, temporalis) can reveal tenderness, hypertrophy, or trigger points indicative of parafunction.
Finally, a diagnostic occlusal analysis may involve mounting diagnostic casts on an articulator using a face-bow transfer. This allows for a static and dynamic analysis of the occlusion outside the mouth, aiding in treatment planning, especially for complex restorative cases. In contemporary practice, digital occlusal analysis systems, like the T-Scan, provide a dynamic, time-based visualization of occlusal contacts, allowing for a more precise quantification of force distribution.
Management of Occlusal Disharmony
The management of occlusal disharmony in periodontics is a staged, strategic process that must always be secondary to the resolution of inflammation. The guiding principle is to create a stable, functional, and non-traumatic occlusal environment that is compatible with the patient’s reduced periodontal support. The therapeutic armamentarium ranges from reversible, conservative adjustments to irreversible, complex restorative interventions.
Phase 1: Anti-inflammatory Therapy – The Indispensable First Step
Before any occlusal intervention is considered, the periodontal inflammation must be controlled. This involves scaling and root planing, patient education, and often antimicrobial therapy. The rationale is twofold. First, much of the tooth mobility and discomfort associated with periodontitis is inflammatory in nature and will diminish as the inflammation resolves. Treating mobility before inflammation control can lead to unnecessary or inappropriate occlusal therapy. Second, performing occlusal adjustment on an inflamed periodontium is akin to adjusting the fit of a shoe on a foot that is actively swelling; the target is unstable. A re-evaluation period of 4-8 weeks post-initial therapy is essential to establish a new baseline for the periodontium.
Phase 2: Definitive Occlusal Therapy
Once inflammation is controlled, the clinician can address the residual occlusal abnormalities. The modalities fall into three main categories: occlusal adjustment, splinting, and occlusal rehabilitation.
1. Occlusal Adjustment (Coronoplasty)
This is the selective reshaping of tooth surfaces to eliminate specific occlusal interferences and create a more favorable force distribution. It is a subtractive, irreversible procedure and should be executed with precision.
-
Indications: Acute TFO (e.g., a high restoration); removal of premature contacts that cause a deflective slide; elimination of balancing side interferences that are deemed destructive in a particular patient; to create mutually protected occlusion (canine guidance) where appropriate; and to reduce the load on a specific tooth with compromised support.
-
Principles: The adjustment follows a systematic sequence, typically starting with the elimination of premature contacts in centric relation, followed by refinement of lateral and protrusive excursive contacts. The use of thin articulating paper (e.g., 8 or 12-micron) is critical to identify precise contact points. The adjustments are performed with fine-grit diamonds or finishing burs, followed by polishing. The process is incremental, often requiring multiple appointments, to avoid creating new interferences or causing dentinal hypersensitivity. The endpoint is an occlusion with even, simultaneous contacts in centric relation/MI, smooth, disclusive excursive movements, and elimination of the specific interferences that were identified as problematic.
2. Occlusal Splinting
Splinting involves joining two or more teeth together to create a rigid or semi-rigid unit. This redistributes occlusal forces across a larger periodontal surface area, thereby reducing the load on any individual compromised tooth. Splints can be temporary (e.g., wire-reinforced composite) or permanent (e.g., cast metal or fiber-reinforced bridges).
-
Indications: To reduce excessive tooth mobility that is causing patient discomfort or functional difficulty; to prevent pathological tooth migration; to stabilize teeth following surgical procedures to promote healing; and as a diagnostic tool to assess if stabilizing a segment improves symptoms before committing to permanent reconstruction.
-
Considerations: Splinting is not a panacea. It simplifies the occlusal environment but does not eliminate the need for occlusal adjustment. Over-splinting can create a rigid lever arm that may transfer excessive forces to the terminal abutments. The decision to splint must be based on a careful risk-benefit analysis, considering the long-term prognosis of the teeth involved and the patient’s ability to maintain oral hygiene around the splint.
3. Occlusal Rehabilitation
This represents the most complex and invasive level of occlusal management. It involves the comprehensive reconstruction of the occlusion through restorations (crowns, onlays, bridges) or orthodontic tooth movement. This approach is indicated when the occlusal disharmony is so severe that it cannot be managed by adjustment or splinting alone.
-
Indications: Severe, generalized occlusal wear; collapsed occlusal vertical dimension; extensive tooth loss requiring replacement; need to establish a completely new occlusal scheme (e.g., converting to canine guidance or group function) in the context of a full-mouth reconstruction; and as part of an implant-supported rehabilitation.
-
Principles: This requires a meticulous interdisciplinary approach. Diagnostic wax-ups, articulated casts, and a trial restoration phase (using provisional restorations) are essential. The provisional phase is critical to test the planned occlusal scheme, vertical dimension, and esthetics before committing to definitive restorations. The occlusion is built to be stable, atraumatic, and maintainable. In cases of severe parafunction, it is often prudent to incorporate an occlusal device (night guard) over the final restorations to protect them from the high forces of bruxism.
The Role of the Occlusal Device (Night Guard / Splint)
The use of a removable occlusal device is one of the most versatile tools in managing occlusal disharmonies, particularly those stemming from parafunction.
-
Stabilization Splints: Typically a hard, full-coverage acrylic appliance worn on the maxillary arch. Its primary role is not to stop bruxism but to provide a stable, flat, and atraumatic surface for the mandibular teeth to contact. This protects the natural dentition from further wear, reduces muscle hyperactivity, and provides the clinician with a diagnostic opportunity to evaluate the patient’s response to an optimized occlusal contact pattern. In periodontics, a stabilization splint can be invaluable for reducing load on compromised teeth, allowing healing, and testing the viability of a new occlusal scheme.
-
Nociceptive Trigeminal Inhibition (NTI) Device: A smaller, anterior-only device that prevents posterior tooth contact. It works by reducing the maximum clenching force, making it effective for patients with severe bruxism and muscle pain. However, its use in periodontics is debated, as it can lead to anterior open bite or over-eruption of posterior teeth if used long-term without supervision.
In all forms of occlusal management, the key is a phased, reversible approach whenever possible. The goal is not to achieve a “textbook” occlusion but to find a stable equilibrium that respects the patient’s adaptive capacity, maintains the gains achieved through anti-inflammatory therapy, and ensures the long-term stability of the dentition.
Recent Techniques to Record Occlusal Disharmonies
The assessment of occlusion has evolved significantly from the subjective interpretation of articulating paper marks. Modern technology offers objective, quantifiable, and dynamic methods for recording occlusal disharmonies, allowing for more precise diagnosis and treatment.
1. Digital Occlusal Analysis (T-Scan)
The T-Scan system (Tekscan, Inc.) is the most significant advancement in occlusal analysis. Unlike articulating paper, which provides only a static, qualitative record of where teeth touch, the T-Scan provides a dynamic, real-time visualization of how and when they touch. It consists of a ultra-thin, disposable sensor that the patient bites on. The sensor records the relative force of each tooth contact over time, displaying the data in a video-like animation.
-
Key Advantages: It identifies the sequence of contacts (which teeth contact first) and the force distribution across the arch. It can quantify occlusal force imbalances, showing if one side of the arch is receiving a disproportionate load. It is particularly useful for identifying occlusal interferences that are not easily seen with paper, such as a “balancing side” interference that appears early in a lateral movement. In periodontics, it allows the clinician to objectively assess if a tooth with reduced support is bearing an excessive load and to verify that an occlusal adjustment has truly balanced the forces, not just redistributed them to another area. The T-Scan provides a level of precision that is unattainable with traditional methods, making it invaluable for complex restorative and implant cases.
2. Computerized Mandibular Scanning (Jaw Tracking)
Systems like Cadiax (Gamma Dental) or Modjaw (Modjaw) use electromagnetic or optical sensors to record the patient’s unique mandibular movements in three dimensions.
-
Application: These systems create a highly accurate, digital dynamic simulation of the patient’s jaw movement. This data can be used to program a virtual articulator, allowing the clinician to design restorations that are perfectly harmonized with the patient’s individual functional movements. This is a leap forward from using average or mechanical articulator settings. For a periodontist, this ensures that a new crown or bridge, which could become a source of iatrogenic TFO if not correctly designed, will be in harmony with the patient’s envelope of motion, minimizing the risk of creating new occlusal interferences.
3. Digital Intraoral Scanning and CAD/CAM Integration
The advent of high-precision intraoral scanners (e.g., iTero, 3Shape TRIOS) has revolutionized occlusal documentation. A digital scan provides a permanent, 3D record of the pre-treatment occlusion. This can be overlaid with scans of the preparation and the planned restoration.
-
Application: In occlusal adjustment, a “pre-op” scan can be compared to a “post-op” scan to precisely quantify how much tooth structure was removed and to ensure that desired contact points were achieved. More importantly, when integrated with CAD/CAM (Computer-Aided Design/Computer-Aided Manufacturing), it allows for the creation of restorations that are digitally designed to fit within the patient’s existing occlusal scheme or a new, pre-determined scheme from a diagnostic wax-up. This reduces the risk of delivering a restoration with a premature contact, a common iatrogenic cause of TFO.
4. Electromyography (EMG) and Bruxism Monitoring
Surface EMG devices (e.g., BTS Bioengineering) can measure the electrical activity of the masticatory muscles, providing objective data on muscle hyperactivity, fatigue, and symmetry. More recently, portable, home-based EMG devices have emerged for the long-term monitoring of bruxism, providing a more accurate picture of a patient’s parafunctional activity than a clinical interview can offer. This data can be used to diagnose the severity of bruxism, guide the selection of occlusal devices, and monitor the efficacy of treatment.
Future Considerations
The future of occlusal considerations in periodontics lies in a paradigm shift from reactive management to predictive, personalized, and preventative care. The integration of advanced diagnostics, digital workflows, and a deeper biological understanding will define this evolution.
One of the most promising frontiers is the development of patient-specific risk assessment models. Currently, the decision to perform occlusal therapy is based on clinical judgment. Future models will integrate objective data from digital occlusal analysis (T-Scan), quantified bruxism activity (portable EMG), 3D radiographic bone volume and morphology (CBCT), and even genetic markers for susceptibility to inflammation or tissue repair. By combining these factors, a “periodontal occlusal risk score” could be generated, allowing clinicians to predict with greater accuracy which patients are most likely to suffer from the co-destructive effects of occlusal forces and would therefore benefit most from proactive intervention.
The rise of artificial intelligence (AI) will be transformative. AI algorithms trained on thousands of clinical cases could analyze a patient’s intraoral scan, radiographs, and occlusal data to automatically identify patterns of occlusal disharmony that are subtle and easily missed by the human eye. AI could suggest optimal occlusal adjustment strategies, predict the long-term stability of a splint or restoration design, and even design a personalized occlusal device optimized for force distribution and patient compliance.
In the realm of treatment, we will likely see the refinement of biologically-oriented occlusal therapy. Instead of a “one-size-fits-all” occlusal scheme, therapy will be tailored to the patient’s individual adaptive capacity. For patients with a robust, healthy periodontium, a wider range of occlusal schemes may be acceptable. For those with a reduced, compromised periodontium, the goal will be to create an ultra-protective occlusal environment, possibly utilizing computer-guided coronoplasty with robotic precision to remove interferences measured in micrometers.
Furthermore, the concept of dynamic monitoring will become standard. With the advent of chairside and home-based sensors, occlusion will no longer be assessed as a static snapshot during a periodic exam. Instead, the patient’s occlusal function and parafunction will be continuously or periodically monitored. This data will be used to create a closed-loop system of care, where the detection of a new occlusal interference or an increase in bruxism activity triggers a preventative intervention, such as a remote adjustment of a 3D-printed occlusal device, before it can lead to clinical pathology.
Ultimately, the future of occlusion in periodontics will be characterized by greater precision, objectivity, and personalization. It will move decisively away from dogmatic principles and towards an evidence-based, biologically-informed approach that leverages technology to preserve the dentition, enhance the outcomes of complex care, and ensure the long-term stability and health of the periodontium.