Introduction to chemotherapeutic agents
Microbial plaque is the primary etiology of periodontal diseases and its removal with mechanical therapy (such as scaling, root planing, and power instrumentation) is considered as a gold standard to achieve periodontal health. In addition to the mechanical therapy, many chemotherapeutic agents, including antimicrobials and host modulation agents have been used to achieve better results. A chemotherapeutic agent is a general term for a chemical substance that provides a clinical benefit. This term does not signify the method by which the agent provides clinical benefit. It may be by reducing or eliminating infective agents such as bacteria, fungi or viruses or by modulation of the host response, reducing tissue damage caused by this response.
Rationale for using chemotherapeutic agents in periodontal diseases
The primary rationale for using chemotherapeutic agents is to eliminate, reduce or alter the effects of microorganisms in the oral cavity and elevated levels of pro-inflammatory mediators. Although, mechanical debridement removes bacterial plaque and debris which are responsible for periodontal breakdown, but some individuals continue to experience periodontal attachment loss even after adequate mechanical debridement. This continued periodontal breakdown has been explained due to the ability of major periodontal pathogens to invade the periodontal soft tissues. It has been shown that various periodontal pathogens such as Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans, Fusobacterium-nucleatum, Treponema denticola, Bacteroides 1, 2 can invade the periodontal soft tissues. Also, the bacterial biofilm may be difficult to ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Another important rationale for using chemotherapeutic agents is poor host defense 3. Patients with acute periodontal diseases such as acute necrotizing ulcerative gingivitis and necrotizing ulcerative periodontitis are candidates which may get benefited from anti-microbial therapy. The success of antimicrobial therapy depends on the susceptibility of bacteria to the antimicrobial agent.
Desired properties of an anti-microbial agent:
1. Effectiveness against specific pathogens.
2. Non-toxic to oral tissues and minimal side effects.
3. Does not cause overgrowth of other microorganisms.
4. Does not contribute to the development of bacterial resistance.
5. Substantiveness (resists dilution).
Classification of anti-microbial agents
The anti-microbial agents can be classified on the basis of their mechanism of action and their spectrum of antimicrobial activity.
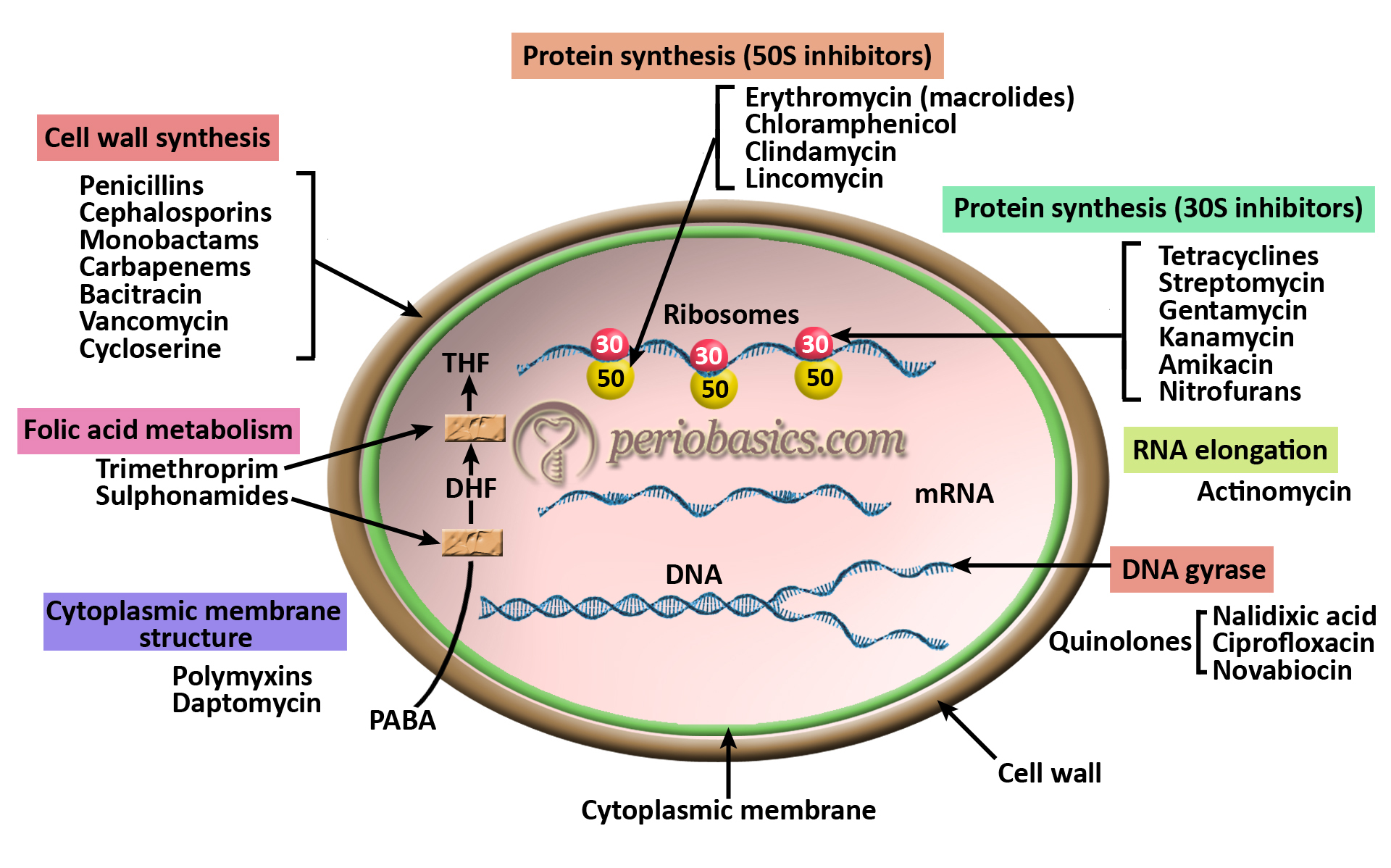
Based on their mechanism of action:
Agents that inhibit synthesis of bacterial cell walls,
Penicillins
Cephalosporins
Monobactams
Agents that interfere with the cell membrane of the micro-organism, affecting permeability,
Some antifungal agents.
Agents that inhibit protein synthesis by affecting the function of the 30S or 50S ribosomal subunits,
Tetracyclines
Macrolides
Clindamycin
Agents that block important metabolic steps of the micro-organisms,
Sulfonamides
Trimethoprim
Agents that interfere with nucleic acid synthesis,
Metronidazole
Quinolones
Based on their spectrum of activity:
Broad-spectrum (active against both Gram-positive and Gram-negative organisms. Examples include: tetracyclines, phenicols, fluoroquinolones, “third-generation” and “fourth-generation” cephalosporins).
Narrow-spectrums (have limited activity and are primarily only useful against particular species of micro-organisms. Example include: Aminoglycosides and sulfonamides, which are effective only against aerobic microorganisms and nitroimidazoles which are generally effective only against anaerobes.)
Antibacterial agents
The most commonly used chemotherapeutic agents in the treatment of periodontal diseases are anti-bacterial agents. Before we discuss these agents, it is important to know the difference between antibiotics and anti-microbial agents. An antibiotic is a low molecular substance produced by a microorganism that at a low concentration inhibits or kills other microorganisms. An antimicrobial is any substance of natural, semisynthetic or synthetic origin that kills or inhibits the growth of microorganisms. All antibiotics are anti-microbials, but not all antimicrobials are antibiotics.
Routes of administration
These agents can be administered systemically or locally (local drug delivery). The most commonly used route of drug administration is the systemic route. The bacteriostatic or bactericidal concentration of anti-microbial agents can be safely achieved by systemic administration of these drugs. The drug can reach the periodontal tissue and pocket via serum and act on bacteria in periodontal tissue and the base of the pocket. Certain drugs like tetracycline, when administered systemically, achieve more concentration in gingival crevicular fluid (GCF) as compared to serum 4. The drug can then bind to the tooth surface, from which it is released in an active form 5. However, systemic administration is associated with side-effects. Further, the bacteria in the biofilm are much more resistant to these antimicrobials because of the protection provided by the protective layer covering the biofilm. The administration of systemic antibiotic therapy should be considered for a particular patient based on its potential benefits and side effects. As already stated, patients with limited response to an adequate mechanical therapy are indicated for systemic antibiotic therapy.
On the other hand, local drug delivery provides a ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Advantages of systemic drug delivery:
1. Antimicrobial activity can be achieved at multiple sites and also at the reservoir sites such as tongue, tonsils and buccal mucosa.
2. The organisms residing at the base of the pocket and in periodontal tissue can be reached.
3. A shorter time of administration.
4. A large number of antimicrobials and their combinations are available for systemic use.
5. Low cost.
Advantages of local drug delivery:
1. It provides a highly concentrated form of the drug without any systemic side effects.
2. Patient compliance is improved.
3. Because of the highly concentrated form of drug, chances of development of resistance are minimal.
Criteria for prescribing antibiotic therapy
There are many factors which should be considered before an antibiotic is prescribed to a patient. These include:
Whom to treat?
The clinical condition of the patient should dictate the need for antibiotic therapy. Patients who do not respond appropriately to standard periodontal treatment such as patients with Grade C (aggressive) periodontitis, patients with refractory periodontitis and acute periodontal lesions such as necrotizing ulcerative gingivitis or periodontitis. In general, patients who demonstrate multiple sites with periodontal pockets ≥ 5 mm and in whom a periodontal infection can be diagnosed are the patients indicated for antibiotic therapy. Most of the clinicians prefer to give systemic antibiotic therapy to a patient scheduled for periodontal surgery.
Microbial culturing and culture sensitivity:
The anti-microbial should be ideally selected on the basis of culturing of the plaque sample obtained from periodontal pocket and its culture sensitivity test. The plaque samples may be obtained from recently active pockets or the pool of plaque samples obtained from deep pockets in different parts of the oral cavity. One advantage of the pooled plaque sample is that the range of periodontal pathogens present in plaque samples against which antimicrobial therapy is required can be determined 6. The plaque sample should be collected before ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Starting the antibiotic therapy:
As already stated, the physical disruption of biofilm is essential to achieve maximum benefit from antibiotic therapy because bacteria in a well-organized biofilm are 500-1000 times more resistant to antibiotics as compared to planktonic bacteria 7. Slots et al. (1999) 8 have reported that the application of anti-infective agents in a systematic manner may promote the results of regenerative therapy. The authors recommended initiating antibiotic course 1-2 days prior to the surgery and continuing it for a total of at least 8 days. However, scientific documentation for the regimen is not available.
Consultation with the patient:
The patient should be explained in detail the need for antibiotic therapy and its potential benefits. The patient should also be explained about the side-effects that are related to the use of a particular antibiotic.
Choice of antibacterial agents for systemic administration:
The choice of an antibiotic ideally depends on the microbial analysis and antibiotic sensitivity test. However, most of the times the choice of antibiotic is made on the basis of clinical signs. The most commonly used antibiotics in periodontal treatment include β-lactams (amoxicillin with or without clavulanic acid), tetracyclines (tetracycline, doxycycline, minocycline), metronidazole and clindamycin. The clinician should be well versed with the pharmacokinetics, pharmacodynamics, and spectrum of action of antibiotics and their rational use in clinical conditions. There are various factors which should be considered while choosing an antibiotic and its dose for a particular patient. These include,
Choosing anti-bacterial agent for empirical therapy:
Most of the times the antibiotics are prescribed based on the clinical presentation of the disease. So, choosing of antibiotic should be evidence-based and according to the patient’s need.
Spectrum of chosen drug:
The spectrum of the drug should include the targeted organism/organisms. In empirical therapy usually, broad-spectrum antibiotics are given so that all suspected organisms are covered, whereas, in rational therapy, a narrow-spectrum drug should be given which targets only the identified organism/organisms.
Age of the patient:
The pharmacokinetics of drugs, to a great extent is dependent upon the age of the patient. In old age, the dose of the drug is usually reduced due to its slow clearance from the body. Use of particular antibiotics may not be suitable for a particular age group. For example, tetracyclines accumulate in the developing teeth and bone, so their use in young children is not recommended.
Status of renal and hepatic function:
The drugs are metabolized mostly in the liver or kidneys. So, the hepatic and renal function have to be considered while prescribing any drug to a patient.
Patients with compromised host response:
In patients who are systemically compromised should be considered for aggressive antibiotic therapy. In an immunocompetent individual, a bacteriostatic antibiotic may be sufficient to control the growth and multiplication of microorganisms, but in an immunocompromised individual, appropriate bactericidal dose of antibiotic is necessary to control the growth and multiplication of microorganisms.
Pregnancy:
All efforts should be done to avoid antibiotic therapy during pregnancy because this may have adverse effects on the developing fetus. However, when required antibiotic should be prescribed following the FDA classification of drugs during pregnancy (See “Periodontal treatment of female patients”).
Patient already taking medications:
Many drugs may have an adverse reaction with each ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Drug allergy:
Allergic reaction to a specific drug may be life-threatening. So, any allergic reaction to a drug should be carefully recorded while taking the case history.
Principles of anti-bacterial drug dosing
The dose of anti-bacterial agent is decided on the basis of its minimum inhibitory concentration (MIC) and gingival fluid concentration (CGCF). MIC90 or minimum inhibitory concentration 90% is the concentration of drug that will inhibit the growth of 90% of the bacterial strains of a species that are tested in vitro. The effectiveness of the drug in periodontal pocket is determined by the relationship between CGCF and MIC90.
100 (CGCF/MIC90) = antimicrobial activity expressed as a percentage for each antibiotic and each organism.
While deciding the dosage of an antibacterial agent, following points should be considered,
- Some anti-bacterial agents require a high concentration of the drug (above MIC) in plasma and tissues for effective bacterial killing. These agents include aminoglycosides, metronidazole, and quinolones. On the other hand, other agents require a prolonged exposure to the bacteria to be effective. These agents include beta-lactams.
- The dosing interval depends on the plasma half-life of the drug. The plasma half-life of the drug, in turn, depends on its pharmacokinetics in the body. Some drugs achieve peak concentration of drug in shorter time duration, while others take more time. A frequency of drug dosing which maintains required levels of the drug in plasma should be considered.
- The loading dose is necessary to quickly achieve the required plasma levels of the drug because after oral administration, it takes 6-12 hours to achieve required plasma and tissue levels of the drug.
- The dose of the drug should achieve 2-8 times the minimal inhibitory concentration of the drug in plasma. This is because tissue barriers may impede the drug penetration into tissues.
- The duration of the therapy should be continued until the infection is significantly resolved. It should allow the host defense system to overcome the infection. For bacteriostatic agents, the duration of therapy is longer as compared to bactericidal agents. As a general rule, antibiotics are usually employed for 48 hours after eliminating signs of an infection. Most periodontal infections can probably be treated in 14 days or less duration of antibiotic therapy 9.
Problems associated with the use of anti-microbial therapy in periodontal diseases
There are some basic problems associated with the use of various anti-microbial agents in periodontal diseases. The first and foremost problem is that periodontal diseases are multi-factorial disease. Although, bacterial etiology is the primary etiology of most of the periodontal diseases, but many systemic, environmental and genetic factors are also associated with periodontal disease progression. The second problem is that multiple microorganisms are associated with periodontal diseases ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book ……..
Commonly used anti-bacterial agents in periodontics
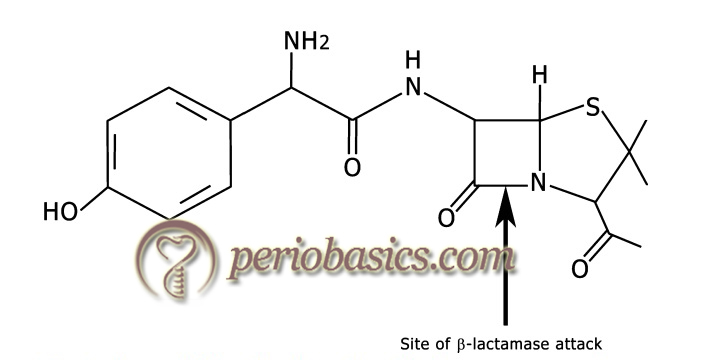
Penicillins:
Penicillin was discovered by Sir Alexander Fleming in 1928 which started a new era of infection control in human history. Penicillins exert their antibacterial action via inhibiting the bacterial cell wall synthesis, resulting in cell death. Structurally, all penicillins are composed of a β-lactam ring, a thiazolidine ring, and an acyl side chain. Various different penicillins have been derived by substituting the acyl side chain in its basic structure. These include benzylpenicillin, phenoxymethylpenicillin, and more broad-spectrum drugs, such as amoxicillin and ampicillin. The variation in the acyl side chain in different penicillins results in significant variations in their properties in terms of improvement in stability to gastric acid, improvement in absorption and higher serum concentrations, and activity against Gram-negative as well as Gram-positive bacteria.
Pharmacokinetics:
Penicillins can be administered both orally and parenterally, but benzylpenicillin can only be given parenterally because it is not stable in acidic medium in the stomach. For oral penicillins (phenoxymethylpenicillin, amoxicillin, and ampicillin), the usual dose is 250 mg every 8 hours. The dose can be increased in severe infections, such as in severe dental infections 3 g loading dose of amoxicillin followed by 8 hourly administration has been recommended 10. Absorption of penicillins takes place in the upper gastrointestinal tract. The absorption rate may get reduced due to the presence of food but amoxicillin is one of the most readily absorbed penicillin. Penicillins get easily distributed in the body, but do not cross the blood-brain barrier because of their lipid insolubility. These get partially bound (46-58%) to proteins and are eliminated from the body via filtration from the kidneys.
| Antibacterial spectrum of various penicillins. | |
|---|---|
| Narrow spectrum penicillins | Penicillin G Penicillin V |
| Broad-spectrum penicillins (aminopenicillins) | Amoxicillin Ampicillin Bacampicillin |
| Penicillinase-resistant penicillins | Cloxacillin Nafcillin Methicillin Dicloxacillin Oxacillin |
| Extended-spectrum penicillins | Carbenicillin Mezlocillin Piperacillin Ticacillin |
| β-lactamase inhibitors | Clavulanic acid Sulbactam Tazobactam |
Antibacterial spectrum:
Penicillin group of drugs consists of many derivatives of penicillin with varying range of the antibacterial spectrum. Some of them are effective against many Gram-positive and Gram-negative bacteria while some are effective against only limited bacterial species.
Mechanism of resistance:
There are three mechanisms by which bacteria offer resistance to penicillins: decreased permeability of the cell wall to the antibiotic, alteration in penicillin-binding proteins and by producing β-lactamases.
Decreased permeability of bacterial cell wall: The structure of the cell wall of Gram-positive and Gram-negative bacteria is different. Antibiotics can easily diffuse through the cell wall of Gram-positive bacteria due to its simple structure made up of peptidoglycan polymer. On the other hand, the bacterial cell wall in Gram-negative bacteria is complex, made up of ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Alteration in penicillin-binding proteins: To exert their bactericidal action, penicillins bind to specific proteins in the bacteria named penicillin-binding proteins. Alteration in these proteins may result in the increased resistance of bacteria to antibiotic. This type of resistance has been observed in methicillin-resistant staphylococci 12 and in penicillin-resistant Gonococcal strains 13.
Production of β-lactamases: This is the most important mechanism of bacterial resistance to penicillins and cephalosporins. The resistance is offered by the production of β-lactamase enzyme which causes hydrolysis of the β-lactam ring, resulting in inactivation of the antibiotic. β-lactamases are produced in large quantity by Gram-positive bacteria as compared to Gram-negative bacteria where these enzymes are found in relatively small amounts primarily located in ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Clinical uses in periodontal diseases:
It has been shown that amoxicillin, ampicillin, and augmentin are effective in refractory periodontitis either used alone 14 or in combination with metronidazole 15. However, most of the periodontal pathogens are Gram-negative and are not sensitive to penicillins so mostly penicillins are used in combination with other drugs which have Gram-negative spectrum. Furthermore, penicillin-resistant organisms do not respond to various penicillins so clavulanic acid is added which neutralizes β-lactamases produced by these organisms.
Adverse effects:
The major side effect associated with the use of penicillins is anaphylaxis and the development of resistance. The anaphylactic reaction is a medical emergency and should be managed appropriately (discussed in detail in “Principles of periodontal surgery”). Other side effects include diarrhea and skin rashes which are more common with ampicillin. In susceptible patients, cross hypersensitivity exists for all penicillins. So, once identified, no derivative of penicillin group should be given to a hypersensitive patient.
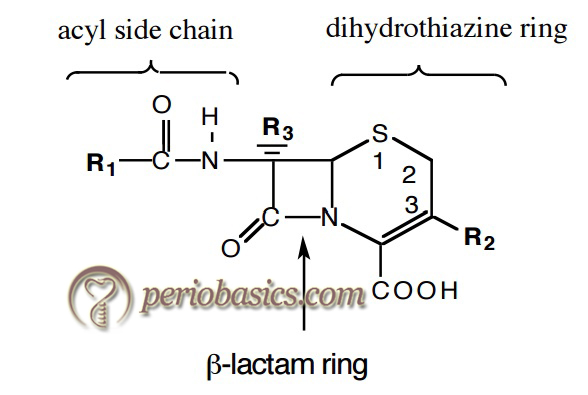
Cephalosporins:
Cephalosporins are β-lactam antibiotics that differ from the penicillins in that the B ring is a 6- membered dihydrothiazine ring. The mechanism of action of cephalosporins is similar to that of penicillin. These bind to the penicillin-binding proteins in the bacterial cell and inhibit cell wall synthesis. In general, cephalosporins are less susceptible to β-lactamases as compared to penicillins. Presently, there are many cephalosporins available which can be classified based on their antibacterial properties and when they were introduced.
Various properties of cephalosporins such as ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Cefazolin:
It is a semisynthetic cephalosporin with broad-spectrum of antibacterial activity. It is specifically used to treat cellulitis, urinary tract infections, pneumonia, endocarditis, joint infection, and biliary tract infections. It is a first-generation cephalosporin antibiotic and similar to other agents in the first generation, it is very effective against Gram-positive bacteria and some Gram-negative bacteria. The drug is not absorbed from the gastrointestinal tract, so, must be administered parenterally. Peak serum concentrations attained 1-2 hours, post intramuscular injection. Cefazolin is excreted unchanged in the urine. In the first six hours, approximately 60% of the drug is excreted in the urine and this increases to 70%-80% within 24 hours. For mild infections, a dose of 250-500 mg every 8 hours is indicated; whereas in moderate to severe infections, 500 mg-1g every 6-8 hours is recommended. In life-threatening infections (e.g., endocarditis, septicemia), 1-1.5 g every 6 hours with a maximum dose of 12g/day is recommended. The common side effects include gastrointesti-nal upset, rash, pruritus and local reactions. Severe effects include anaphylaxis, blood dyscrasias, and markedly elevated liver enzymes. It is contraindicated in patients with known hypersensitivity to penicillin.
Cefadroxil:
It is also a semisynthetic first-generation cephalosporin with antibacterial activity. It binds to and inactivates penicillin-binding proteins (PBPs) located on the inner membrane of the bacterial cell wall. These proteins are responsible for the terminal stages of assembling the bacterial cell wall and in reshaping the cell wall during growth and division. The drug is almost completely absorbed from the gastrointestinal tract. After doses of 500 mg and 1 gm by mouth, peak plasma concentrations of ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Cefalexin:
Cefalexin (also spelled cephalexin) is a beta-lactam antibiotic within the class of first-generation cephalosporins. It is effective against both Gram-positive and Gram-negative organisms. It can be administered in relatively high oral doses without gastrointestinal irritation, and because it is absorbed high in the intestinal tract, it does not disturb the lower bowel flora. The drug is not absorbed from the stomach, but is totally and rapidly absorbed in the upper intestine. There is no appreciable biotransformation of the drug in the liver and the drug is rapidly cleared from the body by the kidneys. 70 to 100% of the dose is found in the urine 6-8 hr after each dose. The mechanism of action is the same as that of penicillin, that is, binding to PBPs and hampering cell wall synthesis.
The drug is indicated for the treatment of respiratory tract infections caused by Streptococcus pneumoniae and Streptococcus pyogenes; otitis media due to Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, Streptococcus pyogenes, and Moraxella catarrhalis; skin and skin structure infections caused by Staphylococcus aureus and/or Streptococcus pyogenes; bone infections caused by ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Cefotaxime:
Cefotaxime is a third-generation semisynthetic cephalosporin antibiotic with bactericidal activity. The mechanism of action is similar to that of penicillin. It has a broad-spectrum activity against Gram-positive and Gram-negative bacteria. A positive feature of cefotaxime is that it displays resistance to penicillinase and is useful to treat infections that are resistant to penicillin derivatives. Approximately 20-36% of an intravenously administered dose of cefotaxime is excreted by the kidney as unchanged cefotaxime and 15-25% as the desacetyl derivative, the major metabolite. The drug is primarily used to treat gonorrhea, meningitis, and severe infections, including infections of the kidney (pyelonephritis) and urinary system. Also used before an operation to prevent infection after surgery. The adverse effects seen following an overdose of the drug include nausea, vomiting, epigastric distress, diarrhea, and convulsions.
Ceftriaxone:
It is a broad-spectrum third-generation cephalosporin antibiotic with a very long half-life and high penetrability to the meninges, eyes and inner ears. The drug is administered intramuscularly or intravenously. After administration, the drug is widely distributed into most body tissues and fluids, including the gallbladder, liver, kidneys, bone, sputum, bile, and pleural and synovial fluids; unlike most other cephalosporins, ceftriaxone has good CSF penetration. Ceftriaxone crosses the placental barrier. Ceftriaxone is partially metabolized in the body and is excreted principally in the urine; some drug is excreted in bile by biliary mechanisms, and small amounts appear in breast milk. Elimination half-life is 51/2 to 11 hours in adults with normal renal function; severe renal disease prolongs half-life only moderately.
Ceftriaxone is highly efficient against streptococci, Haemophilus influenzae, neisseriae, penicillin-resistant strains of Staphylococcus aureus, multiresistant enterobacters, as well as other bacteria. Its effect against ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …....
Ceftazidime:
Ceftazidime is a semisynthetic, broad-spectrum, third-generation cephalosporin. It is used especially for Pseudomonas and other Gram-negative infections in debilitated patients. Compared to the second and first-generation cephalosporins, ceftazidime is more active against Gram-negative bacteria and less active against Gram-positive bacteria. Ceftazidime also crosses the blood-brain barrier and reaches therapeutic concentrations in the CNS. Half-life, following intravenous administration, is approximately 1.9-hours. Since ceftazidime is eliminated almost solely by the kidneys, its serum half-life is significantly prolonged in patients with impaired renal function. The common side effects associated with this drug include nausea, vomiting, elevated liver enzymes, leucopenia, thrombocytopenia, rashes and allergic manifestation. The drug is contraindicated in hypersensitivity to the drug or other cephalosporins. The drug is never administered along with chloramphenicol.
Cefepime:
It is the fourth-generation cephalosporin antibiotic developed in 1994. It has an has an extended spectrum of activity against Gram-positive and Gram-negative bacteria, with greater activity against both Gram-negative and Gram-positive organisms than third-generation agents. Cefepime is usually reserved to treat moderate to severe nosocomial pneumonia, infections caused by multiple-drug-resistant microorganisms (e.g., Pseudomonas aeruginosa) and empirical treatment of febrile neutropenia. It has the same mode of action as other beta-lactam antibiotics (such as penicillins). The drug ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
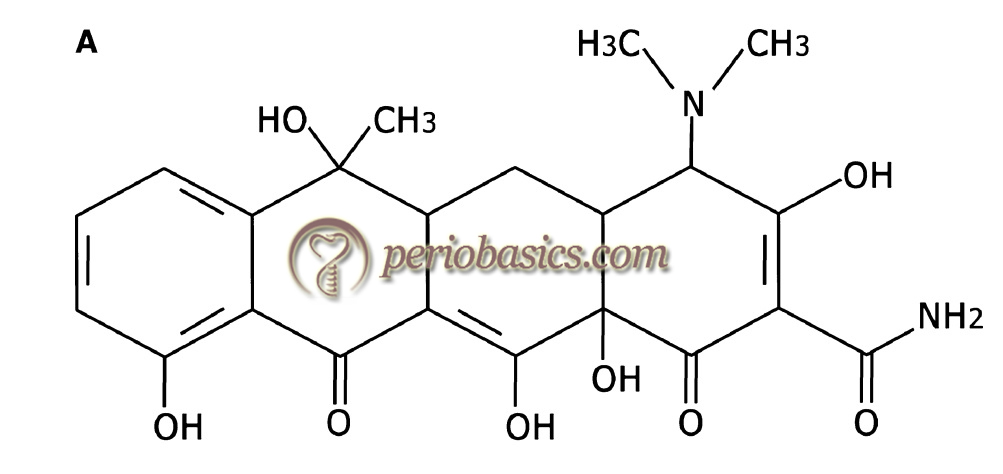
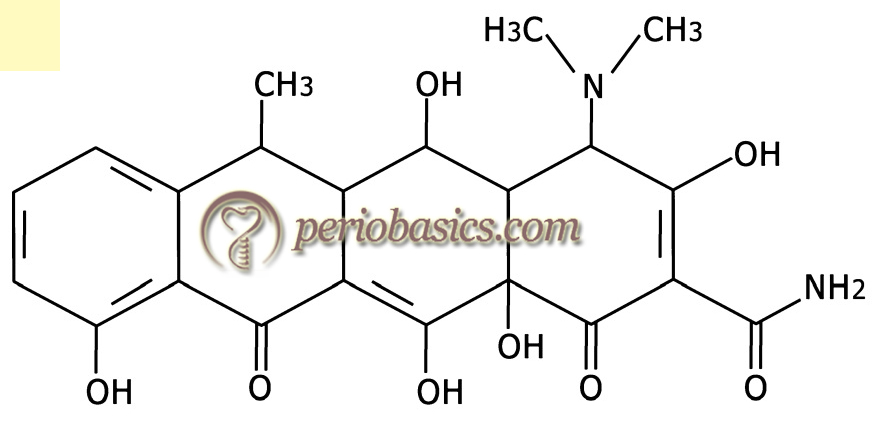
Tetracyclines
Tetracyclines belong to a group of broad-spectrum antibiotics which also includes other antibiotics, namely doxycycline, lymecycline, minocycline, demeclocycline, and oxytetracycline. These are active against both Gram-positive and Gram-negative bacteria. These drugs exert their bacteriostatic action via binding to the bacterial 30S ribosomal subunit and inhibiting protein synthesis. However, when used in a high concentration, such as in local drug delivery, these exert a bactericidal action by their ability to cause alterations in the cytoplasmic membrane. The alterations in the cytoplasmic membrane result in the leakage of the cellular content and finally resulting in cell death. The chemical formula of tetracycline is C22H24N2O8 and that of doxycycline is C22H24N2O8.
Pharmacokinetics:
The most common route of administration of tetracyclines is oral. These are rapidly absorbed from the intestinal tract. Tetracycline should not be taken with milk products or with other substances containing calcium, magnesium, iron, or aluminum because these ions chelate with tetracyclines. The plasma half-life of tetracycline is 6-10 hours and a regular dose of tetracycline is 250 mg at 6-hourly intervals. The GCF concentration achieved is 4-8 μg/ml and plasma concentration achieved is 1.9-2.5 μg/ml 17.
The half-life of doxycycline and minocycline is 16-18 hours and are effective in their action on bacteria due to their high lipid solubility. The loading dose of doxycycline is 200 mg followed by 100 mg daily doses. Furthermore, tetracyclines have the property of binding to the tooth surfaces, from which they may be released slowly over time 18.
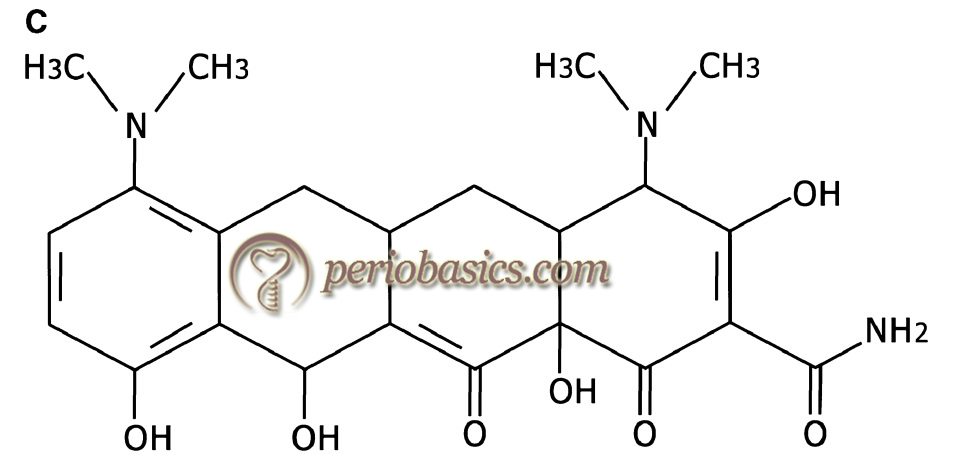
Minocycline is effective against multiple Gram-negative organisms. It is less phototoxic and nephrotoxic as compared to tetracycline. The dosage of minocycline is 100 mg ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Interestingly, after oral dosing, the concentration of tetracycline, minocycline, and doxycycline in GCF can reach a level 10 times and five times in the serum 20, 21. After a regular oral dose, tetracycline achieves a GCF concentration of 2 to 10 μg/mL. The state of renal function affects the clearance of tetracycline so it should not be given to patients whose renal function is compromised. On the other hand, doxycycline is excreted predominantly in the feces so can be given to patients with compromised renal function. Similarly, minocycline is metabolized primarily in the liver and excreted in feces so can be given to patients with compromised renal function.
Antibacterial spectrum:
Tetracyclines are broad-spectrum antibiotics effective against many Gram-positive and Gram-negative bacteria. Tetracycline has been shown to be very effective in the treatment of Grade C periodontitis because Aggregatibacter actinomycetemcomitans, the prime pathogen of Grade C periodontitis is very susceptible to this antibiotic. Because of the tissue invasion property of this microorganism, it is difficult to eliminate just by mechanical debridement alone. It has been demonstrated that 1g/day systemic administration of tetracycline for 3-6 weeks along with adequate plaque control can halt the progression of Grade C periodontitis 22, 23.
Other pharmacological properties of tetracyclines:
In addition to the antimicrobial effect, tetracyclines also exhibit additional pharmacological properties, which are of significance in the management of periodontal diseases. Tetracyclines are capable of inhibiting collagenase 24 due to their property to bind with calcium and zinc ions present on the enzyme. However, this property of tetracyclines depends on the source of the enzyme and type of tetracycline used. Tetracyclines are more effective in neutralizing PMN’s derived MMPs (primarily, MMP8) than fibroblasts, epithelial cells and macrophages derived MMPs (primarily MMP1). Doxycycline is the most effective tetracycline for collagenase inhibition. Sub anti-microbial dose of doxycycline has been used clinically for host modulation (for detail read “Host response modulation therapeutic agents in periodontics”).
Further, tetracyclines may also act as oxygen radical scavengers produced by PMN’s. These oxygen radicals have an ability to activate latent collagenase, thus tetracyclines can prevent the oxidative activation of latent collagenase 25. Along with the inhibition of neutrophil-derived collagenase enzyme, tetracyclines also exert their anti-proteolytic property by preventing the formation of neutrophil-derived reactive oxygen species, i.e., hypochlorous acid, hydrogen peroxide, and hydroxyl radicals 26. Tetracyclines also prevent bone resorption due to their anti-collagenase and anti-proteolytic activity. They have been shown to inhibit osteoblast-derived collagenases and have a modifying effect on osteoclasts 27. Tetracyclines inhibit bone resorption induced by parathyroid hormone 28.
Tetracyclines have been shown to exhibit anti-inflammatory properties. This property of tetracyclines is attributed to their ability to suppress of PMN activity, scavenging reactive oxygen species and ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Mechanism of resistance:
There are primarily three mechanisms, by which bacteria become resistant to tetracyclines: limiting the access of tetracyclines to ribosomes, protection of ribosomes from the drug and tetracycline inactivation by bacteria.
Limiting the access of tetracyclines to ribosomes:
This is accomplished by two mechanisms: reduced uptake of tetracyclines and tetracycline efflux. The entry of tetracyclines in a bacterial cell is required to achieve their antibacterial action via hindering protein synthesis. Some bacteria reduce the entry of tetracyclines by altering the porin proteins (e.g. OmpF) present in the cell wall. It results in increased bacterial resistance up to 6 to 18 fold 32, 33. The second mechanism is expelling the tetracyclines out of the bacterial cell. It is one of the most common mechanisms adopted by microorganisms for drug resistance. Two major efflux systems used for ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Protection of ribosomes from drug:
This is a less common mechanism of bacterial resistance to antibiotics as compared to drug efflux mechanism where specific proteins are synthesized in the cytoplasm which interact and associate with the ribosomes making them insensitive to tetracyclines 35, 36. There are multiple ribosome protection resistance genes which have been characterized and sequenced, including tet(M), tet(O), tet(Q) and tet(S) 37-40.
Tetracycline inactivation:
Resistance genes have been identified in the bacterial cells, which confer resistance to tetracycline by enzymatic degradation of the drug. This type of resistance was first discovered by Guiney et al. (1989) 41 from the obligate anaerobe Bacteroides fragilis.
Clinical use in periodontal diseases:
As already stated, soft tissue invasion by periodontal pathogens makes them inaccessible to mechanical periodontal therapy. Thus, mechanical treatment may not predictably eliminate putative pathogens such as A. actinomycetemcomitans from the subgingival area. It has been demonstrated that tetracyclines have the ability to concentrate in the periodontal tissues and inhibit the growth of A. actinomycetemcomitans 42-44. Furthermore, sub-inhibitory concentrations of tetracyclines have been shown to reduce adherence and co-aggregation of species including P. gingivalis and P. intermedia during plaque formation 45, 46.
However, because of increased bacterial resistance against tetracyclines, a combination of metronidazole and penicillin has been preferred by some investigators. As tetracyclines exhibit host modulation properties, many chemically modified tetracyclines have been used for this purpose. The sub-antimicrobial dose of doxycycline has been used in many clinical trials for host modulation.
Adverse effects:
The most significant unwanted effect of tetracycline is its incorporation into calcifying tissues which causes permanent discoloration of teeth 47. So, it should not be prescribed in children below the age of eight years and in pregnant patients as it gets deposited in teeth and bone. Photosensitivity is another side effect of these drugs so patients are advised to avoid sunlight. The gastrointestinal disturbance is one more side effect which can be seen in some patients. Patients may complain of nausea, vomiting, abdominal discomfort or diarrhea. This is caused primarily due to disturbance of normal gastrointestinal flora. Tetracyclines have also been implicated in causing ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Metronidazole
Metronidazole is a nitroimidazole compound with bactericidal, amoebicidal and trichomoncidal properties. It was initially developed as an antiprotozoal agent. Presently, in dentistry, it is a widely used drug for the treatment of Gram-negative, anaerobic periodontal infections. The exact mode of action has not been fully elucidated but disruption of DNA and inhibition of nucleic acid synthesis seems to be the primary actions of this drug.
Pharmacokinetics:
The commonly used dosage of metronidazole is 200 mg three times a day for 3 days. However, in severe infections 400 mg, twice a day dosage may be used for the duration of 5 days. The drug may be given orally or parenterally. The drug is rapidly absorbed after oral administration and it reaches its peak plasma concentration within 1-2 hours. The plasma half-life of the drug is 8 hours. The drug is metabolized in the liver and has good tissue penetration. It diffuses across the blood-brain barrier, crosses the placenta and appears in the saliva and breast milk. The drug is not significantly bound to plasma proteins. The drug is excreted in urine in an unchanged form.
The drug is contraindicated in patients with evidence of or a history of blood dyscrasias, the presence of active organic disease of the central nervous system and in the case of hypersensitive reaction to the drug. It should also not be given ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Antibacterial spectrum:
The drug is bactericidal and effectively kills many anaerobic Gram-negative bacilli including Bacteroides fragilis and other Bacteroides species and also Fusobacterium species. Along with Gram-negative bacteria, the drug is effective against various Gram-positive bacteria including Clostridium species, Eubacterium, and anaerobic Streptococcus. As already stated, the drug is very effective against pathogenic protozoa, including Trichomonas vaginalis and other Trichomonads and the causative organisms of acute ulcerative gingivitis.
Mechanism of resistance:
Metronidazole has been extensively used but acquired resistance to this drug has rarely been reported. Two mechanisms proposed for increased resistance include reduced entry of the drug into the cell and reduced intracellular reduction of the drug. Production of 5-nitroimidazole reductase which enzymatically reduces the 5-nitroimidazole to a 5-amino derivative is another mechanism by which the drug molecules are inactivated. The genes which code for this enzyme include nimA, nimB, nimC and nimD.
Clinical uses in periodontal diseases:
Metronidazole has been used extensively in the treatment of periodontal infections including, refractory periodontitis 48, 49, adult periodontitis 50, 51 and acute necrotizing ulcerative gingivitis 52, 53. The use of metronidazole in the treatment of periodontitis in the absence of scaling and root planing has been shown to reduce mean probing depths up to 0.4 to 2.4 mm 54. The subgingival bacterial count has also been shown to be reduced, specifically for Spirochetes and Bacteroides 55, 56. Studies have also compared metronidazole monotherapy with mechanical periodontal treatment. These studies have concluded that ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Adverse effects:
The commonly associated adverse effects with the use of this drug are gastrointestinal disturbance, nausea, vomiting, dyspepsia, diarrhea, and constipation. A metallic, sharp unpleasant taste is a common finding. A moderate and transient leukopenia may occasionally be observed in some patients. The most serious neurological side effects of this drug include convulsive seizures, encephalopathy, aseptic meningitis, optic and peripheral neuropathy. Metronidazole can interact with various drugs including coumarin anti-coagulants, disulfiram, alcohol, cyclosporine, phenobarbital, phenytoin etc. Hypersensitivity reaction to this drug have also been reported. Rare adverse effects associated with this drug include burning while urination, bloody or cloudy urine, tachycardia, chest pain and bleeding gums.
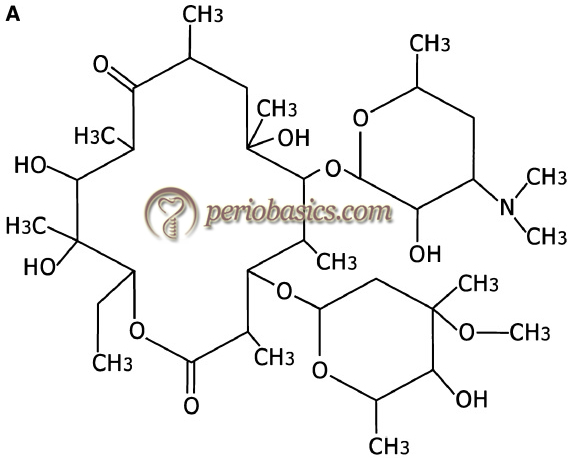
Macrolides
Macrolides are primarily used to control infections caused by Gram-positive bacteria. First macrolide used was erythromycin which is in clinical use for more than 45 years now. Newer macrolides include azithromycin, spiramycin, roxithromycin, and clarithromycin. These drugs inhibit RNA-dependent protein synthesis, resulting in bacteriostatic antimicrobial activity.
Pharmacokinetics:
Erythromycin:
Chemically, erythromycin is C37H67NO13. It is destroyed by gastric acid, except if administered with a protective enteric coating. The drug has a good oral bioavailability but it is affected by food in different ways depending on the formulation used. The absorption of the drug is decreased with the base forms and increased with the estolate form. The drug has a short half-life of 1-1.5 hours and is administered 6 hourly. Erythromycin is highly bound to plasma proteins and gets well distributed in body tissues. The drug is metabolized in the liver with the help of hepatic cytochrome P-450 isozymes. Around 20% of the oral dose of erythromycin is excreted in urine and rest in feces.
Clarithromycin:
It has a good oral bioavailability which does not depend on the presence of food. The drug is rapidly absorbed from the gastrointestinal tract after oral administration. The absolute bioavailability of 250 mg clarithromycin tablets is approximately 50%. The half-life of the drug is 3-7 hours and is administered twice daily. After oral administration, 20-40% of the drug is excreted in urine. In renal dysfunction, the dosage of the drug should be reduced due to decreased drug clearance.
Azithromycin:
Azithromycin is the first of a subclass of macrolides called azalides. Oral bioavailability of the drug is good and is independent of the presence of food. After administering an oral dose of 500 mg, azithromycin is absorbed from the gastro-intestinal tract with an absolute bioavailability of 37%. Therapeutic use requires a single dose of 250 mg/day for 5 days after an initial loading dose of 500 mg. Maximum serum concentration of 0.3 – 0.4 µg/mL is achieved in 2 to 3 hours. The penetration of drug is good, owing to its lipid solubility. It has been proposed that this drug penetrates fibroblasts and phagocytes in concentrations 100-200 times ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book ……..
Spiramycin:
The absolute oral bioavailability of spiramycin is up to 30-40%. It has got an extensive distribution in tissues. Plasma half-life of this drug is 6.2 to 7.7 hours. The drug is usually less metabolized than some other macrolides. The post-antibiotic effect of spiramycin is prolonged as compared to erythromycin against Staphylococcus aureus. Renal excretion of the drug is up to 4-20%. The major route of drug excretion is via bile.
Roxithromycin:
Roxithromycin is absorbed after oral administration with an absolute bioavailability of approximately 50%. The half-life of the drug is 12 hours and is administered twice daily. It is well bound to plasma proteins (92 to 96%). The drug undergoes limited metabolism in the body, presumably in the liver. Approximately 53% of the oral dose of the drug is excreted through feces, approximately 7% of a dose is excreted in the urine and 13% is eliminated via the lungs.
Antibacterial spectrum:
As already stated, macrolides are primarily active against Gram-positive bacteria including Streptococci, Pneumococci, methicillin-sensitive Staphylococci. They have a limited Gram-negative spectrum which includes Bordetella and Campylobacter.
Mechanism of resistance:
There are primarily three mechanisms by which bacterial resistance occurs toward macrolides: efflux of drug from bacterial cell, alterations in ribosomes to prevent effective binding of macrolides and production of enzymes that inactivate the drug.
Efflux of the drug: The efflux pumps effectively transport the drug out of the bacterial cell, thereby providing resistance to the drug. The MEF family genes are associated with the production of these ATP-dependent efflux pumps.
Alterations in ribosomes: The acquisition of one of 21 erm genes by bacteria facilitates the alteration of target ribosomes. The genes code for rRNA methylases which cause methylation ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Enzymatic inactivation of the drug: Production of enzymes by bacteria which degrade the drug is one quite effective mechanism of drug resistance. It has been reported that production of hydrolases, esterases, transferases and phosphorylases result in the inactivation of various macrolides and related molecules 59.
Clinical use in periodontal diseases:
The clinical application of erythromycin in the management of periodontal diseases is limited because it is not effective against many of the periodontal pathogens and it does not concentrate in GCF. Use of azithromycin has been recommended in periodontal infections because it is found to concentrate in the inflamed periodontal tissues. Spiramycin has shown beneficial results when used in periodontal infections. It is excreted in high concentrations in saliva 7. Studies have shown improvement in clinical parameters following administration of spiramycin as an adjunct to scaling and root planing 60.
Adverse effects:
The common side effects associated with the use of macrolides includes cough, fever, general feeling of discomfort or illness, hives, hoarseness, skin rashes, itching, joint or muscle pain and shortness of breath. Rarely abdominal pain, dizziness, drowsiness, headache and burning sensation have been reported.
Clindamycin:
Clindamycin is a lincosamide antibiotic synthesized by chemically modifying the naturally occurring lincomycin. This drug is effective against a wide spectrum of facultative and strictly anaerobic bacteria 61, 62. It exerts its antibacterial action by binding to 50 S subunit of bacterial ribosomes thereby inhibiting protein synthesis. At low concentration, it is bacteriostatic but bactericidal activity is usually achieved with the recommended doses 63.
Pharmacokinetics:
The oral bioavailability of clindamycin is good, with approximately 90% absorption of the drug from the gastrointestinal tract. After doses of 300 and 600 mg, peak plasma concentrations of 4 and 8 μgm/ml, respectively is achieved in the plasma. It is usually given in a dosage of 150 mg thrice a day for 10 to 12 days. Clindamycin is widely distributed in body fluids and tissues including bone. However, the drug does not reach the cerebrospinal fluid in significant concentrations. The drug is ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Anti-bacterial spectrum:
Clindamycin is primarily active against anaerobic infections including Porphyromonas species, Prevotella species, Bacteroides fragilis group, Veillonella species, and Fusobacterium species, including β-lactamase producing strains. It is also effective against Gram-positive organisms including Actinomyces, Eubacterium, Lactobacillus, Peptostreptococcus, Propionibacterium, and Staphylococcus species, including penicillin-resistant strains 64-66. Along with its anti-bacterial effects clindamycin also reduces adherence of bacteria to the epithelial cells of mucosal surfaces and inhibits the expression of virulence factors 67, 68. It has been shown to inhibit the production of M protein by group A β-hemolytic streptococci.
Clinical use is periodontal diseases:
Many studies have demonstrated the beneficial effects of clindamycin as an adjunct to scaling 69, 70. Clindamycin has been shown to be useful in periodontal infections. Long-term beneficial results have been observed with clindamycin dos-age of 600 mg/day for 7 days in refractory periodontitis cases 70-72. One year post-treatment results with clindamycin have been shown to be superior when compared to tetracycline 73.
Adverse effects:
Acute pseudomembranous colitis is the major concern with the use of clindamycin. The condition develops as a result of proliferation of the antibiotic-resistant Clostridium difficile, which produces metabolites toxic to the gut wall, resulting in ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Aminoglycosides
Aminoglycoside antibiotics are widely used for the treatment of severe Gram-negative infections, often in combination with a β-lactam antibiotic. These are among the most rapidly acting bactericidal drugs available for the treatment of aerobic Gram-negative sepsis. These are bactericidal and perform bacterial killing in dose-dependent manner. It must be noted here that antibiotics with concentration-dependent killing characteristically kill bacteria at a faster rate when drug concentrations are higher. Commonly used aminoglycosides include gentamicin, tobramycin, netilmicin, and amikacin. The mechanism of action of aminoglycosides is via binding to the 30S ribosomal subunit which causes inhibition of protein synthesis and misreading of mRNA, resulting in dysfunctional protein production.
Pharmacokinetics:
Aminoglycosides are primarily used for parenteral therapy. The minimum inhibitory concentration (MIC) of amikacin is more than other aminoglycosides. As the pharmacokinetics of all the aminoglycosides is similar, so more dose of amikacin is required to treat the infection. These are usually administered in 8 hourly doses. These drugs have a reasonable distribution into ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Antibacterial spectrum:
Aminoglycosides have a broad Gram-negative spectrum. Gentamicin is quite effective against various Gram-negative organisms including Pseudomonas aeruginosa. Amikacin is the aminoglycoside most resistant to enzymatic inactivation that is why it must be reserved for treating infections due to microorganisms that are resistant to other aminoglycosides. On the other hand, aminoglycosides have a limited spectrum against Gram-positive organisms. These are active against few Gram-positive bacteria including Staphylococci and Streptococci. Some of the aminoglycosides are active against mycobacteria. However, they have no activity against anaerobes.
Clinical use in periodontal infections:
As already stated aminoglycosides have bactericidal, concentration-dependent killing action and are active against a wide range of aerobic Gram-negative bacilli. However, because these are the drug of choice for serious, life-threatening Gram-negative infections, these should not be used during routine periodontal treatment.
Adverse effects:
All aminoglycosides are potentially ototoxic and nephrotoxic and these adverse effects are more pronounced in patients of advanced age, and those with renal impairment, hearing loss or vestibular impairment. Patients with renal disorders must be kept under observation if these drugs are used.
Fluoroquinolones
These are nalidixic acid derivatives, having bactericidal activity. Most commonly used drugs in this group are ciprofloxacin, norfloxacin, ofloxacin, levofloxacin, and gatifloxacin. These drugs perform bacterial killing by inhibiting DNA gyrase and topoisomerase IV 74.
Pharmacokinetics:
The oral absorption of fluoroquinolones is rapid. The serum and urine concentrations of these drugs markedly exceed the MICs for many common bacterial pathogens. The drugs are distributed well in tissues. Various drugs in this group have a different half-life, degree of absorption, metabolism, and elimination. In general, quinolones exhibit linear ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Antibacterial spectrum:
Fluoroquinolones are effective against a wide range of both Gram-positive and Gram-negative microorganisms. Ciprofloxacin, levofloxacin, and gatifloxacin, all have excellent in vitro activity against Enterobacteriaceae, fastidious Gram-negative species such as H. influenzae and other Haemophilus species, N. gonorrhoeae, N. meningitides, and M. catarrhalis. They are effective against many established periodontal pathogens including A. actinomycetemcomitans 75. Ciprofloxacin is effectively used against facultative and aerobic Gram-negative rods and cocci.
Clinical use in periodontal diseases:
Studies have been done to evaluate the efficacy of various fluoroquinolones in the elimination of periodontal pathogens. In a study, it was observed that treatment with ofloxacin in conjunction with open flap surgery was able to suppress A. actinomycetemcomitans below detectable levels for 12 months 76. Fluoroquinolones have been found beneficial in the treatment of A. actinomycetemcomitans associated periodontitis 77.
Adverse effects:
The common side effects associated with the use of these drugs are nausea, vomiting, diarrhea and painful oral mucosa. Pseudomembranous colitis has been observed in patients taking a high dosage of fluoroquinolones. In some patient hypersensitivity reactions such as rashes, pruritus, urticaria, pigmentation and edema of lips have been reported. Ciprofloxacin should not be prescribed to children and young individuals due to potential joint problems.
Vancomycin
It is a glycoprotein antibiotic used primarily to treat Gram-positive infections. The drug is effective against methicillin-resistant Staphylococci and ampicillin-resistant Enterococci. It is a bactericidal drug and performs bacterial killing based on time-dependent or concentration-independent bacterial killing. At high ……….. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Pharmacokinetics:
The drug is administered as a short-term (1 hour) intravenous infusion because it is not appreciably absorbed orally. The plasma half-life of the drug is 6-12 hours. Protein binding of the drug ranges from 10-50%. Factors that affect the overall activity of vancomycin include its tissue distribution, inoculum size, and protein-binding effects. The drug effectively penetrates most of the tissues but is somewhat dependent on the degree of inflammation present. Vancomycin is primarily eliminated via the renal route, with >80%-90% recovered unchanged in urine within 24 h after the administration of a single dose.
Anti-bacterial spectrum and use in periodontal diseases:
Vancomycin is primarily a drug of choice for the elimination of methicillin-resistant strains of Staphylococcus aureus and is generally reserved for serious drug-resistant Gram-positive infections. Its use during routine periodontal therapy is not recommended. Vancomycin is used prophylactically for the prevention of infective endocarditis in patients with prosthetic heart valves.
Adverse effects:
An allergic reaction may occur due to vancomycin which may manifest as pruritus and flushing on the face (Red man’s syndrome), neck, and shoulders. Other adverse effects include reversible neutropenia and thrombocytopenia. Nephrotoxicity may occur if a higher dose of the drug is given or the drug is given in combination with aminoglycosides. Rarely, ototoxicity has been observed, especially when the drug is combined with other ototoxic drugs.
Combination therapy
Beneficial results can be obtained by combining various antibacterial agents. It broadens the anti-bacterial spectrum as compared to that achieved by a single antibiotic. As a rule, the bactericidal drug should not be combined with a bacteriostatic agent because bactericidal agent exerts activity during cell division that is impaired by a bacteriostatic drug. For example, a combination of penicillin and tetracycline is not recommended because former is bactericidal and later is bacteriostatic. Furthermore, anti-bacterial drugs with similar mechanism of action should not be combined. For example, erythromycin or azithromycin should be given concurrently with clindamycin because all of them have a similar mode of action.
The most frequently used combination is that of penicillins and metronidazole. This combination has been used extensively for the treatment of A. actinomycetemcomitans associated localized juvenile periodontitis, Papillon-Lefevre syndrome periodontitis, adult-type periodontitis, rapidly progressing periodontitis, generalized advanced periodontitis, and refractory periodontitis 15, 78-80. This combination has also been shown to be effective in the elimination of P. intermedia 15, 78, 79 in cases of Grade C (aggressive) periodontitis 81. In refractory periodontitis cases, a combination of Metronidazole-Augmentin has been shown to be effective 82. Due to an extensive study by van Winkelhoff et al. (1989) 78, metronidazole and amoxicillin combination has been coined the “van Winkelhoff cocktail”.
Another combination antibiotic therapy for periodontitis is metronidazole and ciprofloxacin. In a study by Slots et al. (1990) 17, it was shown that quite effective in inhibiting enteric rods and Pseudomonas, as well as against A. actinomycetemcomitans, Eikenella corrrodens, Capnocytophaga, and Staphylococci. However, it was found to be ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
The combination of spiramycin and metronidazole is also effective in inhibiting the periodontal pathogens. It has been demonstrated that both Spiramycin and metronidazole have good antimicrobial activity against species of Prevotella, Eubacterium, Peptostreptococcus, Bacteroides, and Porphyromonas, as well as the anaerobic spirochetes 84, 85. However, approximately 90% of A. actinomycetemcomitans strains are slightly resistant to spiramycin and 72% to metronidazole 86.
Sequencing the administration of antibiotics
The antibiotics can be administered one after another to minimize the risk of antagonism between bacteriostatic and bactericidal antibiotics. Although not widely accepted clinically, this method of administration has also been researched. Serial drug regimen investigated for periodontitis includes systemic doxycycline administered initially, followed by either Augmentin or metronidazole 3. Matisko et al. (1992, 1993) 87, 88 used a sequential antibiotic regimen on periodontitis patients, which included ……….. Contents available in the book ……. Con Contents available in the book ……. Contents available in the book ……. Contents available in the book …….
Local drug delivery
The local administration of the antibacterial agents has many advantages over the systemic drug delivery. There has been much advancement in the field of local drug delivery in periodontal therapy. A detailed description of agents used in local drug delivery has been given in, “Local drug delivery in periodontics”.
Other anti-microbial agents used in periodontal therapy
There are many other anti-microbial agents used in periodontal therapy including chlorhexidine, povidone iodine, listerine, sodium hypochlorite, hydrogen peroxide etc. Chlorhexidine is the most common agent used for plaque control. It is considered as a gold standard for chemical plaque control. Subgingival irrigation with chlorhexidine and povidone-iodine has been shown to reduce the subgingival bacterial load. A detailed description of these agents has been given in “Chemical plaque control”.
Other chemotherapeutic agents used in periodontal therapy are host response modulation agents. These agents modulate the host response in such a way that the host-mediated connective tissue destruction is prevented. These agents have been discussed in detail in “Host response modulation therapeutic agents in periodontics”.
Conclusion
Application of chemotherapeutic agents in the overall management of periodontal diseases has been a part of the standard periodontal treatment plan for many years now. However, periodontal infections involve a variety of pathogens with different antimicrobial sensitivities and resistance patterns. The reduction of this bacterial load by mechanical plaque control is the primary treatment in preventing periodontal disease progression and the chemotherapeutic agents can only be used as an adjunct to this treatment. The antimicrobial regimen must be determined carefully depending on the clinical presentation of the disease and the most probable microorganisms involved. Furthermore, unnecessary use of these agents may result in the development of resistance to ensure the survival of that species which then may become difficult to treat. Hence, a judicial use of anti-microbials is recommended. In the next article, we shall read about the local drug delivery.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.