Dental implant therapy
Dental implant therapy has provided us with one of the most promising tooth replacement procedures. Over the last few decades, there has been an increasing use of endosseous (in-bone) implants as a means of providing a foundation for intra-oral prosthetic devices 1, from full arch dentures to single crowns or other devices for orthodontic anchorage 2 or distraction osteogenesis 3,4. Although dental implants are known for a long time, but most of the research and developments in this field have occurred in last few decades. In the following articles we shall read about various aspects of implant therapy, but before moving forward we should remember that every effort should be made to save the natural tooth. In situations where tooth can’t be saved because it has a bad prognosis or cases where teeth have already been extracted, we consider implant therapy as one of our options for treatment.
By definition, implant dentistry is the field of dentistry concerned with the diagnosis, design, and insertion of implant devices and implant restorations that provide adequate function, comfort, and esthetics for the edentulous or partially edentulous patient 5. Before we actually start placing implants in patients, it is important to know the basics of implant therapy. We must be aware of the biological aspect of the implants, the clinical aspect of the implants and most importantly the complications that may occur during the implant therapy and how to handle them. As the patient is paying good money for this treatment, he/she expects esthetically and functionally good dentition. Failing in achieving, what has been told to the patient, may be problematic. So, the patient should be told, exactly what can be achieved practically after the treatment. The patient should not have misconceptions in his/her mind.
The most important step in implant therapy is the diagnosis and treatment planning. Proper knowledge of the bone response, osseointegration, implant surface properties, healing around implants and mechanical forces on implants during function is essential before we start doing implant therapy. It is important to note that any implanted implant/ biomaterial often induces the formation of a poorly vascularized collagenous capsule that can eventually lead to implant failure. Our aim during implant placement is to achieve an environment where bone growth takes place with minimal fibrous growth.
Both surgical and post-surgical phases of implant treatment are equally important. However, it should be remembered that surgical therapy is comparatively a smaller part of the complete implant therapy. The major part of the whole implant treatment is the prosthetic rehabilitation and occlusal harmonization; especially in case of full mouth rehabilitation, where a stable occlusion is mandatory to achieve the long-term stability of the dentition.
Rationale for dental implant treatment
Loss of teeth due to any reason cause compromised chewing ability, speech, facial appearance, and self-confidence. Due to tooth loss, atrophy of the surrounding bone takes place due to lack of use. Dental implants maintain the bone levels by applying direct forces on the bone 6. This is in comparison to removable partial and complete dentures which have opposite effects on bone levels. It has been shown that poorly fitting partial and complete dentures lead to bone resorption as only 10% of the chewing efficiency is achieved by these, causing gradual bone loss 7.
Another important factor is sunken face due to tooth loss. Due to the loss of teeth, muscles of mastication undergo atrophy because of lack of use, giving the patient a sunken face appearance. Dental implants allow the patient to use their muscles of mastication properly, thereby preventing atrophy of these muscles. Dental implants are the closest replacement of natural teeth. The patient’s self-confidence is drastically improved when he/she knows that his/her teeth are fixed and functionally and esthetically good. With implants supported teeth, patients are able to smile with confidence, without worry of denture displacement or showing gaps when smiling. Most importantly, the implant becomes a part of the body after osseointegration. The prosthesis supported by the implant may get deteriorated over time demanding a replacement, but a properly osseointegrated implant may last lifelong.
Classification of dental implants
Based on the implant design:
Sub-periosteal.
Transosteal.
Endodontal.
Intramucosal.
Endosteal:
Ramus frame.
Root form.
Plate form.
Based on the attachment mechanism of the implant
Osseointegration.
Fibrointegration.
Based on macroscopic body design
Hollow dental implants.
Cylindrical dental implants.
Vented dental implants.
Threaded dental implants.
Based on the surface of the implant
Machined surface implants.
Textured surface implants.
Coated surface implant.
Based on the type of the material
Biotolerant.
Bioinert.
Bioactive.
The detailed description of the above classification is given in their relevant topics.
Why titanium?
It is required that the material for dental implants is biocompatible, it must not be toxic and it may not cause allergic reactions 8. It must have a high ultimate strength (Rm) and yield value (Rp) at low density and low modulus of elasticity (E) 9. Although many metal alloys such as alloys of stainless steels, cobalt alloys, titanium (coarse-grained) and titanium alloys have been investigated for their use as dental implants, titanium, and its alloys are mostly commonly used for this purpose 10. So, why do titanium and its alloys show such good biocompatibility as compared to other alloys? Let us try to find out the answer to this question.
Pure Titanium is a highly reactive metal and will react within microseconds to form an oxide layer when exposed to the atmosphere 11. This oxide, which is primarily TiO2, forms readily because it has one of the highest heats of reaction known (ΔH = -915 kJ/mole) (for 298.16°-2,000°K) 12. The formation of its oxide layer makes titanium one of the most passive metals. Although the standard electrode potential was reported in the range from -1.2 to -2.0 volts for the Ti→Ti3+ electrode reaction 13, due to a strong chemical affinity for oxygen, it easily produces a compact oxide film, ensuring high corrosion resistance of the metal. The passive film of TiO2 that forms on titanium is stable, even in biological systems, including chemical and mechanical environments 14.
The easiest method for checking whether the oxide layer formed is protective or not is by calculating Pilling-Bedworth (P-B) ratio 15. In metals where P-B ratio is less than 1 (since the oxide occupies a smaller volume than the metal), the formed oxide is porous and non-protective. But, if it is larger than 2 (since the oxide occupies a large volume and may flake from the surface, exposing fresh substrate surface), it again exhibits non-protectiveness. So, in metals where P-B ratio is between 1 to 2, the volume of oxide is similar to that of metal, so that the formed oxide is adherent to the substrate, nonporous, and protective. For titanium, P-B ratio is 1.76 indicating that TiO2 layer formed on titanium surface is highly protective. The “natural” oxide film on titanium ranges in thickness from 2 to 7 nm, depending on parameters such as the composition of the metal and surrounding medium, the maximum temperature reached during the working of the metal, surface finish, etc. It must also be noted that when the implant is placed in the bone, the oxide layer formed on titanium implants grows and takes up minerals (P, Ca, and S) from the surrounding environment 16, 17.
Factors that affect the biological acceptability and integration of implant are dependent upon the properties of the oxide layer, such as stoichiometry, defect density, crystal structure and orientation, surface defects, and impurities 17, 18. Titanium oxide has a low solubility and an isoelectric point between 3.5 and 6.7 19. This makes the surface only slightly negatively charged at physiological pH, which is thought to reduce the ability for capsule formation after insertion into bone and is also thought to lead to favorable reactions with biomolecules.
Importance of implant surface properties
Because the implant surface is in physical and chemical contact with the surrounding environment, it plays a crucial role in biological interactions for four reasons 20-24:
- It is the only part contacting with the bio-environment.
- The morphology and composition of the surface region of an implanted biomaterial are almost always different from the rest of the implant bulk.
- For biomaterials that do not release or leak biologically active or toxic substance, the characteristics of the surface govern the biological response (foreign material vs. host tissue).
- Surface properties of implants such as topography affect the mechanical stability of the implant-tissue interface.
How the implant surface is modified and how it improves the biological and mechanical properties of dental implants have been discussed in detail in “Dental implant surface treatments”.
Terminologies used in implant dentistry
Before we go ahead with detailed implantology, we must know the terms that are frequently used in implantology. Following is the description of these terminologies,
Implant:
Material inserted or grafted into tissue.
Dental implant:
A permucosal device that is biocompatible and biofunctional, and is placed on or within the bone associated with the oral cavity to provide support for fixed or removable prostheses.
Titanium:
Metal (chemical symbol Ti) having low density, good strength, and corrosion-resistant properties.
Implant fixture/body:
Implant fixture or body is the portion of the implant that is designed to be placed into the bone.
Osseointegration:
Contact established without the interposition of nonbony tissue between normal remodeled bone and an implant at the light microscopic level, entailing a sustained transfer and distribution of load from the implant to and within the bone tissue.
Transosseous implant:
A machined implant consisting of a lower plate fixated under the mandible with pins projecting through the mandible which penetrates into the oral cavity.
Blade implant:
An endosteal implant consisting of an abutment, cervix, and body (or infrastructure) that is thin buccolingually and has fenestrations to permit the ingrowth of the bone/connective tissue for the purpose of anchorage.
Disc implant:
An endosteal design consisting of a thin, plate-like component placed into a horizontal osteotomy and attached to a post-like vertical component that protrudes permucosally.
Cylinder implant:
A round endosteal implant either threaded or press-fit.
Eposteal implant
Device that receives its primary bone support by means of resting upon bone.
Root form endosteal dental implant:
Root-shaped implants that derive their support from a vertical expanse of bone; implants are in the form of spirals, cones, rhomboids, and cylinders; they can be smooth, fluted, finned, threaded, perforated, solid, hollow, or vented; they can be coated or textured and are available to be used as submerged and non-submerged forms in a variety of biocompatible materials.
Endodontic endosteal implant:
A smooth or threaded pin implant that extends through the root into the periapical bone to stabilize a mobile tooth.
Abutment:
It is that part of the implant that lies between the implant and the crown. Abutment screws into the implant fixture.
Abutment screw:
The screw that clamps the abutment onto the implant.
Healing screw:
The final intra-implant screw placed after first-stage surgery.
Healing abutment:
A temporary abutment that is placed after the implant has been inserted and is removed before the permanent restoration is placed.
Osteotomy:
A hole in the alveolar bone made by an implant drill for the placement of a dental implant.
One-stage implants:
Implants that are exposed to the oral cavity after a single surgical procedure.
Two-stage implants:
Implants that are submerged below the gingiva immediately after placement. Second surgery is necessary to uncover them.
Implant exposure:
Exposure of the dental implants which is carried out approximately 4 months after the initial implant placement.
Implant analog:
The implant analog is used by the lab technician during fabrication of the prosthesis. The abutment is attached to the analog and impression is poured. Now, analog replicates the implant in the cast over which the prosthesis is fabricated.
UCLA abutment:
A custom-made abutment designed to be placed on single implants that lack anti-rotational elements.
Long screws:
These are long screws used for attachment of abutment to the implant during open impression technique.
Interim prosthesis:
A fixed or removable dental prosthesis, or maxillofacial prosthesis, designed to enhance esthetics, stabilization and/or function for a limited period of time, after which it is to be replaced by a definitive dental or maxillofacial prosthesis.
Cemented prosthesis
A restoration that is cemented onto the abutment.
Hybrid prosthesis:
It is a prosthesis that is composed of different materials. More specifically, in implant dentistry, the term hybrid implies a combination of a metal framework with a complete denture.
Screw retained prosthesis:
A prosthesis that is attached to the implants with the help of screws and is not cemented.
Implant-retained fixed overdenture:
It is a non-removable prosthesis that attaches to 4, 6 or 8 implants.
Implant-stabilized removable ball overdenture:
A removable prosthesis containing ball attachments to hold, or stabilize the denture in place.
Implant-stabilized removable bar overdenture:
A removable prosthesis containing a bar attachment to hold, or stabilize the denture in place.
Dolder bar:
A connector of multiple prosthetic elements designed to lend strength as well as to retain an overdenture or superstructure; special clips are available that grasp these bars.
Hex-lock:
A 6-sided screwdriver; a matching screw.
Connecting bar:
A fixed bar that connects 2 or more permucosal extensions; in the case of the ramus frame or subperiosteal implant, it can be an integral part of the substructure.
Trephine:
A surgical instrument used for cutting out circular sections. Used to retrieve implant/fractured implant portion.
Vitalium:
Trademark name for a dental alloy comprised of cobalt, chromium, and molybdenum.
Dehiscence, implant:
A splitting open or a break in the covering epithelium, leaving an isolated area of an implant or bone exposed to the oral cavity.
Depassivation:
Local conditions that produce an acidic environment at the metallic interface, causing the metallic oxide to break down.
Coatings:
Layers of materials designed to cover implant substrates for the purposes of making them more biocompatible.
Hydroxyapatite (HA):
Calcium phosphate complex that is a primary mineral component of bone; sprayed-on coating used on early dental implants.
Tricalcium phosphate:
An inorganic, particulate, or solid form of relatively biodegradable ceramic that is used as a scaffold for bone regeneration; it can act as a matrix for new bone growth.
Plasma spray-coated with titanium:
A technique of reliably coating the surface of a titanium implant with small, irregular particles of the same metal.
Resonance frequency analysis (RFA):
Technique for clinical measurement of implant stability/ mobility. A measurement is registered from a transducer attached to the abutment or implant. The device records the resonance frequency arising from the implant-bone interface (change in amplitude over induced frequency band).
Tissue punch technique:
Circular incision made in the soft tissue over a submerged dental implant, manually or mechanically, of a diameter similar to the implant platform. This results in the exposure of the implant by the removal of a circular piece of soft tissue.
Stereolithographic guide:
A drilling guide generated from a computer-aided manu-facturing (CAM), according to information derived from a software-based planning, used for dental implant placement in vivo.
Three-dimensional printing:
A category of rapid prototyping technology. A three-dimensional object is created by layering and connecting successive cross sections of material from information derived from a computed tomography scan. It is used for surgical planning and the generation of a surgical guide.
Multi-unit abutment (MUA):
Designed for screw-retained restorations of partially edentulous and edentulous arches, available in straight and angulated options with a range of collar heights to match the vertical thickness of the soft tissue.
Titanium alloy (Ti-6Al-4V):
A biocompatible medical alloy used for the fabrication of dental implants and their components. Its physical properties are superior to most commercially pure titaniums. The most common titanium alloy used for the fabrication of dental implants is Ti-6Al-4V, which contains approximately 90% titanium, 6% aluminum, and 4% vanadium.
Zirconium (Zr):
A steel-gray hard ductile metallic element with a high melting point that occurs widely in combined forms. It is highly resistant to corrosion, and is used especially in alloys and in refractories and ceramics.
Zirconia abutment:
An esthetic alternative to metal implant abutments due to the white color of zirconia. Zirconia abutments can be custom milled, or stock abutments from a specific manufacturer, available in a variety of configurations with or without pre-machined margins.
Tomogram:
A type of x-ray revealing a particular layer or “slice” of the mouth while blurring out other layers. This x-ray examines structures that are difficult to clearly see because other nearby structures are superimposed, blocking the view.
Distraction osteogenesis:
An invasive surgical technique using specialized instruments which permits bones to become lengthened to as much as 500 μm per day.
Pterygoid implant:
A root-form dental implant that has its origin in the region of the former second maxillary molar and its end point encroaches in the scaphoid fossa of the sphenoid bone. The implant follows an intrasinusal trajectory in a dorsal and mesio-cranial direction, perforating the posterior sinusal wall and the pterygoid plates.
Peri-implantitis:
An equivalent to periodontitis, manifesting around dental implants; bone loss around implants due to bacterial pathogens.
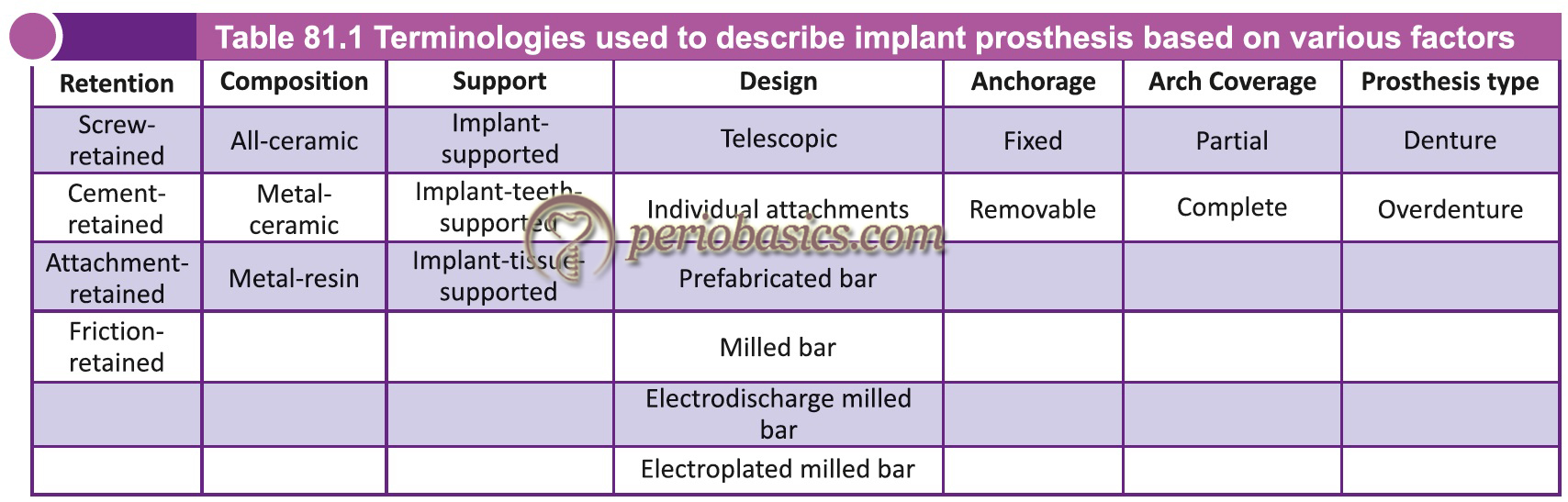
Simplification of implant-supported prosthesis-related terminologies
To simplify the description of implant-supported prosthesis-related terminologies, the implant-supported prosthesis can be described on the basis of various factors as follows,
- Retention.
- Composition.
- Support.
- Design.
- Anchorage.
- Coverage.
- Prosthesis type.
Following table describes the information of an implant prosthesis based on above terminologies.
Conclusion
Dental implant treatment has become the treatment of choice for partially and completely edentulous patients. There has been a tremendous research in implantology in the last few decades. In the present chapter, we have discussed terminologies that are used in implant dentistry. The knowledge these terminologies is important before we go ahead with the discussion on different aspects of implant dentistry. In the upcoming chapters, we shall discuss in detail various aspects of dental implant therapy including diagnosis, clinical and radiographic examination of an implant patient, the procedure for placing implant/implants and its associated complications.
References
References are available in the hard-copy of the website.