Introduction to occlusion
Occlusion plays an important role in the pathogenesis of periodontal diseases. A faulty occlusion may induce traumatic lesions in the supporting periodontal structures, thereby adversely affecting the long-term prognosis of tooth/teeth. Occlusion may also indirectly affect the periodontal health status by interfering with the plaque elimination and by influencing periodontal defense mechanism. Sometimes, occlusal problems are difficult to diagnose and if diagnosed, they may be difficult to treat. Presently, most of the dentists overlook the occlusal disturbances even after they have been recognized. Reason being, most of the occlusal disturbances involve the function of the entire dentition rather than a single tooth or segment. It must be understood that most of the occlusal problems require full mouth treatment and a dentist should be well trained to recognize them and treat them appropriately.
There are many controversies regarding the relationship of occlusal trauma and progression of periodontal inflammatory diseases. Can occlusal trauma initiate gingivitis or periodontitis? Can it modify the response of periodontium to local irritants which are considered as primary etiological factors for periodontal inflammation or their occurrence together is just coincidental? A thorough knowledge of normal occlusion is essential to answer the above questions.
Rationale for comprehensive occlusal examination
A detailed history of the patient and thorough clinical examination are the most fundamental steps in comprehensive periodontal treatment. It must be remembered that occlusal problems are not always associated with pain. It has been demonstrated that individuals with malocclusion have no more pain than those with an ideal occlusal scheme 1-3. It is commonly seen that patients who have severe malocclusion have negligible clinical symptoms. Parafunctional habits are more responsible for causing occlusal and temporomandibular joint problems than a bad occlusion. Lytle et al. (1990, 2001a, 2001b) 4-6 have categorized parafunctional activity, according to the severity of the condition. So, carefully identifying any sign or symptom which is related to occlusal disharmony is the primary rationale of comprehensive occlusal examination.
| Categories of parafunctional activity. | |
|---|---|
| Type 1: | Almost no parafunction, no evidence of wear, mobility, tooth migration, muscle soreness, fractures, cracks, craze lines, or abfractive lesions. |
| Type 2: | Moderate parafunction, evidence of slight wear, mobility, tooth migration, muscle soreness, fractures, cracks, craze lines, or abfractive lesions. |
| Type 3: | Destructive parafunction, evidence of excessive wear, mobility, tooth migration, muscle soreness, fractures, cracks, craze lines, or abfractive lesions. |
Physiology of temporomandibular joint (TMJ)
TMJ is one of the most complex joints in the human body. It is a ginglymoarthrodial joint, a term that is derived from ‘ginglymus’, meaning a hinge joint, allowing motion only backward and forward in one plane, and ‘arthrodia, meaning a joint of which permits a gliding motion of the surfaces 7. Its compound articulation is formed by the articular surfaces of the temporal bone and the mandibular condyle. Both the articulating surfaces are covered by a dense articular fibrocartilage. The right and left TMJs make a bicondylar articulation and an ellipsoid variety of synovial joints.
Components of the temporomandibular joint
TMJ consists of,
- 2 bones: Temporal and mandibular bone.
- A disk that divides the joint into 2 spaces: Upper and lower compartments.
- A joint capsule.
- Ligaments: The lateral ligament, sphenomandibular ligament, and stylomandibular ligament.
- 4 main muscles that create 5 motions: Temporalis, masseter, medial pterygoid, lateral pterygoid.
Bones:
The TMJ is formed by mandibular and temporal bones. The cranial end of ramus of the mandible has two processes: the coronoid process, anteriorly and the condylar process, posteriorly which has a head on top and a distinct neck below. The head of the condyle articulates with the articular surface in the squamous portion of temporal bone. The squamous portion of temporal bone has a concave articular fossa posteriorly and a convex articular tubercle anteriorly.
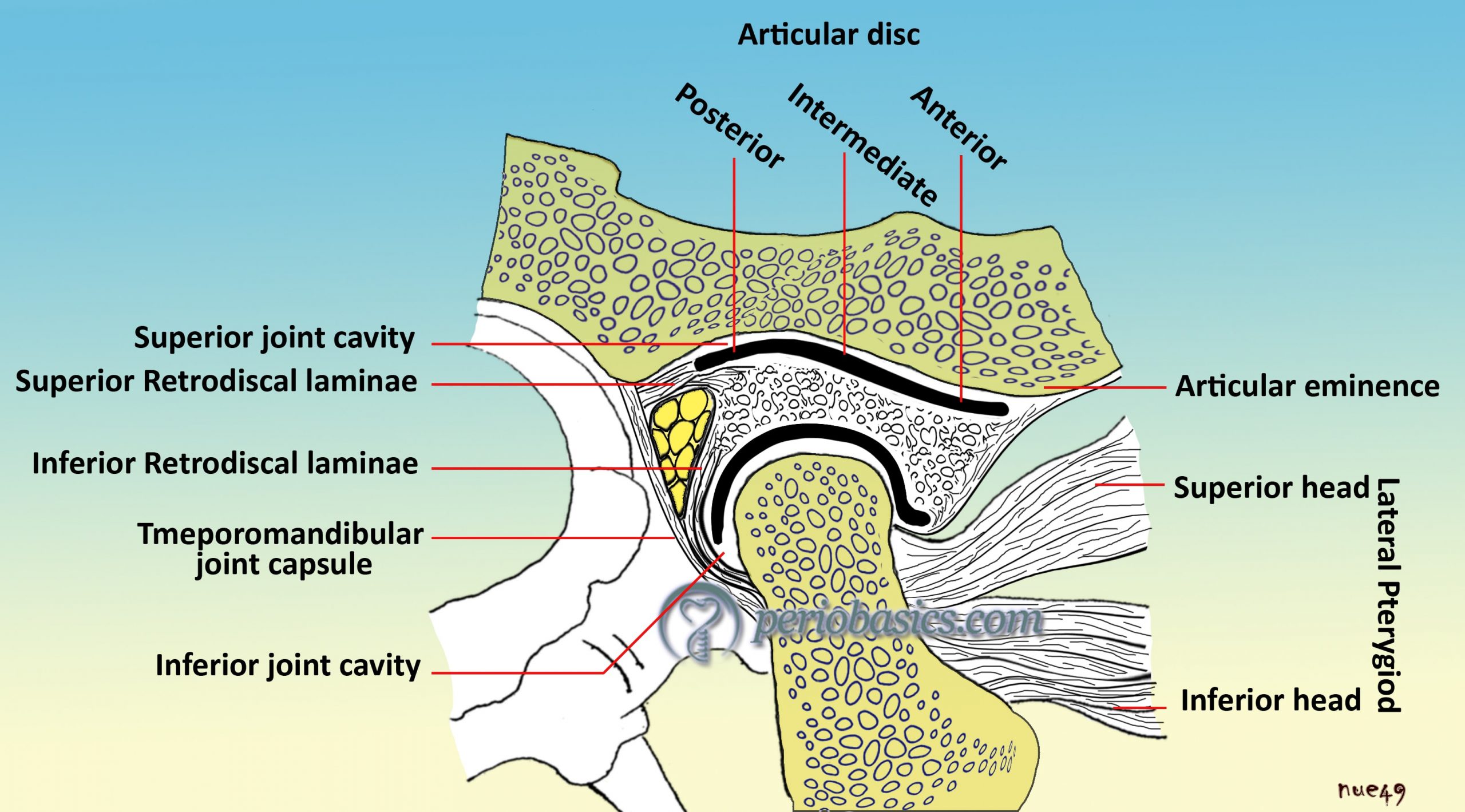
Intra-articular meniscus or disk:
The articular disc of the TMJ is a strong fibroelastic oval disc that is concave inferiorly and concavoconvex above. It consists of strong collagen fibers with a blend of elastic fibers, especially in its anterior and posterior aspects. Unlike other joint discs, it does not have any cartilage in its composition. The disc is attached peripherally to the joint capsule and completely separates the capsule into superior and inferior spaces. It is strongly bound to the lateral and medial aspects of the mandibular condyle and closely tracks the movement of the condyle. The articular disk has 3 bands: anterior (2 mm), middle (1 mm) and posterior (3 mm) band. It is attached to the medial and lateral collateral ligaments laterally. In the bilaminar zone, the disk is ……….. Contents available in the book…………. Contents available in the book…………. Contents available in the book…………. Contents available in the book……..

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
The joint capsule:
The joint capsule completely covers the joint and is wide and loose on the upper aspect around the mandibular fossa and funnel-shaped near the neck of the mandible.
Ligaments:
The TMJ is stabilized by three ligaments: collateral (discal), capsular, and temporomandibular. The lateral ligaments attach the medial and lateral borders of the disc to the condyle. They divide the condyle into two cavities and restrict movement of the disc away from condyle. The capsular ligament surrounds the joint space and disc and acts to contain the synovial fluid within the joint space. The two extracapsular ligaments, sphenomandibular and stylomandibular ligaments act as “guiding” restraints to keep the condyle, disc, and temporal bone firmly opposed. The stylomandibular ligament is, in fact, a specialized band of deep cerebral fascia with thickening of the parotid fascia.
Muscles:
Muscles that are involved in the mandibular movement are masseter, temporal and pterygoid muscles. The masseter muscle has superficial and deep fibers. The superficial fibers originate from anterior 2/3rd of the lower border of the zygomatic arch whereas deep fibers originate from posterior 1/3rd and medial surface of the zygomatic arch. Insertion of superficial fibers is at the angle of the mandible and of deep fibers is at the ramus of the mandible. The temporalis muscle originates from entire temporal fossa and gets inserted into the coronoid process of the mandible. We have two pterygoid muscles: medial and lateral. The medial pterygoid muscle originates from pterygoid fossa of the sphenoid bone and gets inserted at the angle of the mandible on the medial side of the ramus. The lateral pterygoid has two origins. The superior head originates from the greater wing of the sphenoid bone and the inferior head originates from the lateral surface of the lateral pterygoid plate of the sphenoid bone. Insertion of the superior head is at the neck of the condyle and of the inferior head is into the capsule of the TMJ.
| Various mandibular movements and muscles involved in those movements. | |
|---|---|
| Action | Muscles |
| Depression (Open mouth) | Lateral pterygoid Suprahyoid Infrahyoid |
| Elevation (Close mouth) | Temporalis Masseter Medial pterygoid |
| Protrusion (Protrude chin) | Masseter (superficial fibers) Lateral pterygoid Medial pterygoid |
| Retrusion (Retrude chin) | Temporalis Masseter (deep fibers) |
| Side-to-side movements (grinding and chewing) | Temporalis on the same side Pterygoid muscles of opposite side Masseter |
What is occlusion?
Dental occlusion is defined by the Glossary of Prosthodontic Terms as “the static relationship between the incising or masticating surfaces of the maxillary and mandibular teeth or tooth analog” 8. Many books have been written solely on occlusion. Readers are advised to go through these books for a detailed knowledge on occlusion. In the present discussion, we shall discuss normal occlusion in brief, and occlusal interferences in detail. We must know some terminologies before we go ahead with our discussion. These are,
Centric occlusion (CO):
It refers to the relationship of the mandible to the maxilla when the teeth are in maximum occlusal contact, irrespective of the position or alignment of the condyle-disk assemblies.
Centric relation (CR):
It is the position of the mandible when the condyles are in an orthopedically stable position. This occurs when the condyles are in their most superoanterior position, resting on the posterior slopes of the articular eminences with the disks properly interposed.
or
It is the maxillomandibular relationship in which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterior-superior position against the slopes of the articular eminences. This position is independent of tooth contact and is also referred to as retruded contact position (RCP).
Working side:
The side towards which the mandible moves in a lateral movement. Working side condyle pivots within the socket and is better supported.
Balancing side:
It is the non-functioning side from which the mandible moves during the working bite. Balancing side condyle has a downward orbiting path. It is traveling a greater distance in ‘space’ and is more prone to injury or damage.
Terminal hinge position:
It is the most retruded physiological position of the condyle in the glenoid fossa that the patient can achieve with his/her own musculature. In this movement, the mandible turns without any translator component in an arc whose axis lies in the condyle. The importance of this position is that the patient who is edentulous or deprived of cuspal guidance can be trained to repeatedly go through this movement so that patient can duplicate the movement again and again. During the movement, the repeatable reference points can be established and can be used for mounting the casts on articulators.
Static occlusion:
Static occlusion refers to the contact between teeth when the jaw is closed and stationary.
Dynamic occlusion:
Dynamic occlusion refers to the occlusal contacts made when the jaw is moving, as while chewing.
Incisal guidance:
The guidance provided by the palatal surfaces of the maxillary incisors in protrusive movements of the mandible.
Canine guidance:
The guidance provided during the movement of the mandibular canines over the palatal surfaces of the maxillary canines.
Group function:
Multiple contacts between the maxillary and mandibular teeth on the working side during lateral movements.
Christensen’s phenomenon:
A gap which appears between the posterior teeth of opposing dental arches when the mandible is protruded and the incisors are placed in edge-to-edge position.
Curve of Monson:
The curve of occlusion of natural teeth in which each cusp and incisal edge touches or conforms to a segment of the surface of a sphere with its center in the region of glabella.
Curve of Spee:
An arc of a circle that touches the tips of all the mandibular teeth when the skull is viewed laterally; when continued it touches the anterior surface of the condyles.
Normal functional occlusion
Before we start discussing the occlusal abnormalities and interferences, let us first know what all clinical findings are present in normal occlusion. There is a disagreement over defining a normal functional occlusion. Most of the researchers have agreed on the fact that a wide range of malocclusions may be considered normal if they do not possess any subjective symptom or any pathological change due to occlusal disharmony. Further, an occlusion which is otherwise having characteristics of normal occlusion can be considered abnormal if signs and symptoms of occlusal disharmony are present. It is essential for us to know the characteristics of normal occlusion. Andrews (1972) reported six significant characteristics of normal occlusion 9. These are,
1. Molar relationship:
The mesiobuccal cusp of the upper first molar should occlude in the buccal groove of the lower first molar and the teeth are arranged in a smoothly curving line of occlusion. The distal surface of the distobuccal cusp of the upper first permanent molar should make contact and occlude with the mesial surface of the mesiobuccal cusp of the lower second molar.
2. Correct crown angulation (mesiodistal tip of the crown):
The angulation of the facial axis of every clinical crown should be positive i.e. the gingival portions of long axis of all crowns are more distal than the incisal portions. The extent of angulation varies according to tooth type.
3. Correct crown inclination (labiolingual or bucco-lingual torque):
In upper incisors, the gingival portion of the crown’s labial surface is lingual to the incisal portion. In all other crowns, including lower incisors, the gingival portion of the labial or buccal surface is labial or buccal to the incisal or occlusal portion. In upper posterior crowns (cuspids through molars), the lingual crown inclination of the buccal surfaces is slightly more pronounced in the molars than it is in cuspids and bicuspids. In lower posterior crowns (cuspids through molars), lingual inclination progressively increases.
4. Absence of rotations:
Teeth should be free of undesirable rotations.
5. Tight proximal contacts:
In the absence of abnormalities such as genuine tooth size discrepancies, contact point should be tight.
6. Occlusal plane:
The plane of occlusion varies from generally flat to a slight curve of Spee.
To understand occlusion, the first step is to understand the border movements of the mandible and its physiologic functional movements. This is a very vast topic for discussion; however, in the following section, we shall discuss these movements briefly.
Functional movements of the mandible
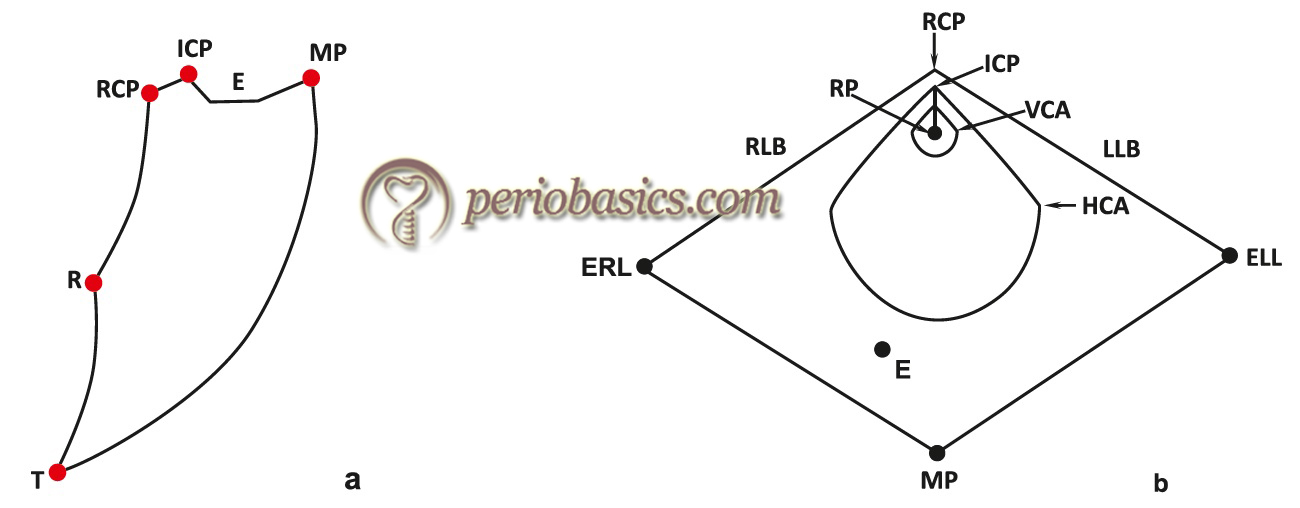
The movement of the mandible during mastication follows a path which is specific for every individual because every individual has a specific occlusal scheme. Posselt in 1957 10 described the extreme or border movements of the mandible as an “envelope of motion”. The positions of the mandible during these border movements are constant and can be reproduced for each individual in both sagittal and horizontal planes. All the mandibular movements which constitute the normal function are within this envelope.
In the facial skeleton, the mandible is the only bone which is movable. The border movements of the mandible are recorded as the movement of the tip of the lower incisor when viewed in the sagittal or frontal plane. When the mandible is opened, the initial movement that occurs along the TMJ is hinge movement. During this movement, the condyles are in retruded and most superior position in their fossae.
When the mandible is moved to make tooth contact, the mandibular position when the first tooth contact occurs is referred to as retruded contact position (RCP)/centric relation (CR). Following this contact, the mandible moves forward to bring the teeth into maximum intercuspation, referred to as intercuspal position (ICP)/centric occlusion (CO). The discrepancy ……….. Contents available in the book…………. Contents available in the book…………. Contents available in the book…………. Contents available in the book……..
The border movements of the mandible can be demonstrated by tracing the movements of the lower incisors when viewed in the sagittal, frontal or horizontal plane.
Mandibular border movement during maximum mouth opening:
While moving the mandible to the maximum mouth opening position, the mandibular movement starts from RCP. Initially, mandible moves in an arc of a circle around the terminal hinge axis. This movement is approximately up to 2-2.5 cm of opening. After this limit, lateral pterygoid muscle is activated which initiates forward translatory movement of the mandible. During translatory movement, condyles slide downwards and forwards along the articular eminences of the glenoid fossae to a point of maximum opening. The most common error done by the dentists during identification of occlusal interferences is the inability to accurately recognize RCP and transferring this registered position to an articulator.
Protrusive mandibular border movement:
When the mandible is moved anteriorly from ICP, it is known as protrusion. The path of this movement is primarily determined by articulating surfaces of anterior teeth. It is referred to as anterior guidance. The anterior guidance is absent if maxillary and mandibular anterior teeth do not come in contact at all (open bite) or if they are in an edge to edge relation. In these cases, the anterior guidance is obtained from the posterior teeth that ……….. Contents available in the book…………. Contents available in the book…………. Contents available in the book…………. Contents available in the book……..
Lateral mandibular border movements:
To understand the lateral mandibular border movements we must know about supporting and non-supporting cusps in the maxillary and mandibular arch. When in ICP, the palatal cusps of the maxillary teeth and buccal cusps of mandibular teeth are referred to as supporting cusps because these contact the cuspal inclines and fossae of the teeth in opposite arch. On the other hand, the buccal cusps of maxillary teeth and lingual cusps of mandibular teeth are referred to as non-supporting cusps. This relationship is reversed in cross bite. To perform lateral mandibular border movement, the mandible is moved to one side by performing lateral excursion and moving it to maximum lateral position without producing any pain. The side to which the mandible is moved is called as working side and the another side is referred to as the balancing side. During registration of lateral movement, the dentist should manipulate the mandible in such as way that any anterior translation of the working condyle is prevented.
While performing this movement; if only canines come in contact on the working side, the occlusion is referred to as canine guided occlusion. On the other hand, if two or more pairs of teeth contact during this movement, the occlusion is referred to as group function occlusion.
Various concepts of mandibular positions
Various authors have different views concerning centric occlusion (CO) and centric relation (CR) positions during mandibular movement. Some authors say that the CO and CR position should coincide 12 while others say that CR and CO positions in natural dentition should not coincide 13. Many researchers believe that the mandibular shift from CO to CR position can be ignored if it is less than 1 mm 11. Presently, most of the researchers believe that CR and CO positions of the mandible should coincide. However, most of the individuals have a slight shift of the mandible from CR to CO position. If this movement is slight (less than 1 mm) with no lateral shift, it should be considered normal. While making occlusal contacts, there should be no deflecting interferences. If these interferences are present, they should be removed. In natural dentition, cuspids should most preferably cause slight disocclusion of both the working and the non-working sides during the lateral mandibular excursion. While doing the protrusive movement, preferably no posterior teeth should come in contact or there should be no deflective contacts.
Conclusion
Occlusion plays a very important role in the maintenance of periodontal health. A harmonious occlusion is a must requirement for a health periodontium. Occlusal disharmonies cause multiple periodontal problems which make it difficult for the individual to perform normal functions like chewing the food etc. In the above discussion, we discussed the physiological aspect of the occlusion as well as the terminologies used to describe various components of occlusion. In the next article “Principles of occlusal therapy”, we shall read about various steps in occlusal harmonization.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.