Introduction to scaling and root planing
The periodontal treatment is initiated with the removal of bacterial deposits and calculus from the tooth surfaces to obtain a biologically acceptable root surface. At the same time, every effort is made to protect the healthy periodontal tissue from any damage. Supra- and subgingival scaling is a routine procedure carried out to achieve a tooth surface free of plaque and calculus and helping in self-performed plaque control by the patient.
Need to eliminate plaque and calculus around the teeth
It has been shown that after a thorough oral prophylaxis, the biofilm formation starts within a few hours on the tooth surface. Within another 48 hours, as the biofilm matures, periodontopathic anaerobes are established initiating gingivitis 1. As the plaque matures, more and more Gram-negative bacteria are established in the dental biofilm initiating periodontal destruction. A host response is generated against these bacteria which causes the production of cytokines, prostaglandins, and chemokines by various inflammatory cells, leading to inflammation and bone loss 2.
Dental calculus is calcified plaque which provides a …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Power-driven scalers
There are two basic types of scalers: manual and power-driven. The manual scalers have been discussed in detail in “Periodontal instruments”. The power-driven scalers are of two types: sonic and ultrasonic. Before we discuss these scalers, we should know the following terminologies,
Frequency:
It is the number of times per second the tip of the scaler moves back and forth during one cycle of orbital, elliptical or linear motion. It is measured in kilohertz (KHz) in scalers. The frequency determines the active area of the tip. Higher the frequency lesser is the active area of the scaler tip.
| Scaler frequency and associated tip movement | |
|---|---|
| Scaler frequency | Active tip |
| 25 KHz | Terminal 4.3 mm |
| 30KHz | Terminal 4.2 mm |
| 50 KHz | Terminal 2.3 mm |
Stroke:
It is the maximum distance to which the tip of the scaler moves during one cycle.
Amplitude:
It is half the distance of one stroke. In recent ultrasonic scalers, the amplitude can be increased or decreased by increasing or decreasing the power setting. At higher power setting, longer strokes are produced while at a lower power setting, smaller strokes are produced with the frequency being constant.
Sonic scalers
The sonic scalers operate at a lower frequency of about 6,000 to 8,000 cycles/second (6-8 KHz). These are air-driven, in which tip of the scaler moves in an orbital motion. The sonic handpiece consists of a hollow rod, a rotor, and several rubber “O” rings. The compressed air is forced through the hollow rod. The rotor is a 6 mm wide ring that surrounds the hollow rod above a series of angled holes present on it. The air forced through the rod escapes through these holes and causes the rotor to …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Advantages:
- They create less heat at the scaling tip than an ultrasonic machine.
- Used with air pressure so no need for separate installation as in the case of ultrasonic scalers.
Disadvantages:
- They are noisy during use.
- These scalers have a low range of vibration and high tip amplitude as compared to ultrasonic scalers.
- A low range of vibration and high tip amplitude hardly ever leads to cavitation of the water jet.
Ultrasonic scalers
In 1880 Pierre and Jacques Curie found that crystals of various materials placed under mechanical stresses develop electrical charges on their surfaces. This conversion of mechanical energy into electrical energy is called the ‘piezoelectric effect’. Conversely, if alternating current at high frequency is applied to a piezoelectric substance, the corresponding lengthening and shortening of the substance over tiny distances result in physical vibrations 3. From 1920 to 1955 many substances such as quartz, barium titanate, lead zirconate titanate, Rochelle salts, lithium sulfate and ferromagnetic metals were shown to have this property.
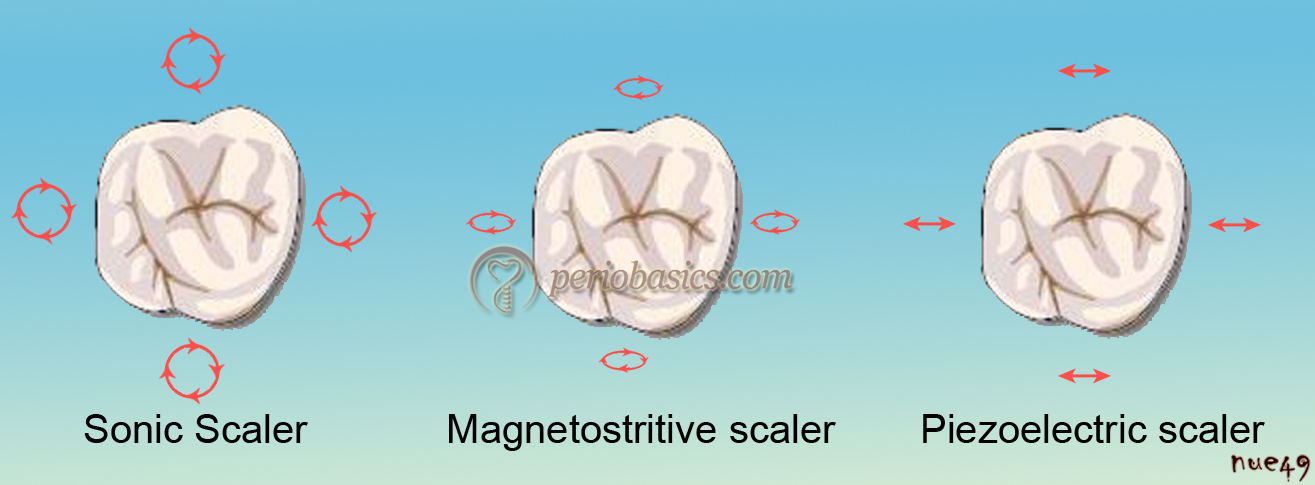
The ultrasonic scalers utilize either magnetostrictive or piezoelectric technology. Magnetostrictive scalers operate at 25,000 to 30,000 cycles/second (25-30 KHz) and have an elliptical motion of the scaler tip, whereas, piezoelectric scalers operate at 28,000 to 36,000 cycles/second (28-36 KHz) and the movement of the tip is in a back-and-forth motion and works along the side of the tooth, shaving off calculus and debris.
Magnetostrictive scalers:
These scalers have a metal stack consisting of nickel-iron alloy strips or a ferrite insert inserted in the handpiece. A live coil is present inside the handpiece that generates an alternating electromagnetic field which causes expansion or contraction of the ferromagnetic material. This results in vibrations which are conducted to the scaler tip. Depending on the type of the instrument, oscillations with constant amplitude up to 100 μm are produced with a frequency ranging from 18 to 45 kHz with most of the units working at 25 or 30 kHz.

Piezoelectric scalers:
In piezoelectric scalers, vibrations are produced due to dimensional changes in quartz crystals housed within the hand-piece as electricity is passed over the surface of the crystals. The ultrasonic energy thus generated, is transmitted via a transducer contained in the handpiece and is prolonged by an amplifier. These units operate at a frequency ranging from 25-50 kHz with most of the units working usually at 28-36 KHz.

Cavitation effect:
A unique property of ultrasonic scalers is cavitation effect. It is a continuous spectrum of bubble activity in a liquid medium in an acoustic field. It ranges from the gentle linear pulsation of gas-filled bodies in low amplitude sound fields to violent and destructive behavior of vapors-filled cavities in high amplitude sound fields 4. Based on these physical properties, cavitation is divided into two types: stable and inertial cavitation 5.
The scaler produces an ultrasound field comprising of a series of compressions and rarefactions (regions of high and low pressure) which cause small bubbles, trapped in the water, to expand and contract. Bubbles produced by inertial cavitation oscillate violently and may expand many times of their original size before imploding. A shock wave is formed when these bubbles …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Acoustic streaming:
Acoustic streaming is characterized by the production of large shear forces in a fluid environment. A complex steady state streaming pattern within the liquid close to the bubble surface is produced due to the rapid cyclical volume pulsation of a gas bubble. The factors on which acoustic streaming depends are displacement amplitude, tip orientation, and the presence of water medium. It increases with increasing displacement amplitude, although it also depends on tip geometry, tip orientation, and distance from the oscillating tip 8.
Acoustic streaming can disrupt the subgingival biofilms associated with periodontal diseases, but along with this, it has been shown that it may also disrupt the blood flow and cells such as human platelets exposed to probes operating at 20 kHz 8. At higher frequencies, it may cause thrombosis in vessels due to platelet aggregation 9.
How to use sonic and ultrasonic scalers?
The scaling unit should be thoroughly disinfected before usage. All the components which can be autoclaved such as the handpiece and tips should be autoclaved before each use. The scaling unit is covered by a plastic barrier. The handpiece and water lines are flushed for 2 minutes to reduce the number of microorganisms in the line. The patient is asked to rinse the mouth for 1 minute with an anti-microbial agent such as 0.12% chlorhexidine to reduce the bacterial load in the oral cavity. Clinician and the assistant should wear protective glasses and high-speed evacuation is used to reduce aerosol contamination.

The sonic and ultrasonic scalers are used with a totally different technique as compared to hand instruments. Most commonly contra-angular curved scaler tips are used for debridement in these scalers. The respective tip is aligned to the tooth in such a way that the convex working end touches the root surface. For exclusive biofilm removal, especially during the maintenance phase the force applied to the scaler tip should be as low as 1 N (feather touch) with the instrument aligned parallel to the tooth surface 10-12. While using the scaler, firstly, the tip of the insert should be used in a probe-like manner to evaluate the morphology and dimensions of the periodontal pocket. Then the tip is moved in a systematic way performing serpentine-like overlapping tractions. After completion of scaling and root planing, the root surface is evaluated with the help of a fine explorer. If any …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Literature review on the comparison between manual and powered scaling instruments
Scaling efficiency and surface roughness:
Several studies have evaluated the scaling efficiency and amount of tooth structure removed mechanically by hand instruments 13-15 and ultrasonic scalers 16, 17. Many studies 18-20 have suggested that hand instruments produce a significantly smoother root surface than ultrasonic scalers, whereas other studies 21 suggested that an ultrasonic scaler produced a smoother root surface than hand instruments. These studies may have contradictory results, but one common finding is that one of the important factors determining the surface smoothness is the efficiency and appropriate technique of scaling used by the operator.
One study compared the scaling efficiencies and root surface roughness after scaling by hand instruments, sonic scalers, and ultrasonic scalers. One study compared a sonic instrument (Periosonic), magnetostrictive ultrasonic (Cavi-tron®, Slimline inserts), and hand curettes to evaluate the removal of plaque biofilm and loss of tooth structure. It was found that all three were effective in disrupting biofilm and in removing biofilm and calculus deposits. Use of the magnetostrictive ultrasonic scaler resulted in the least tooth substance loss 22.
Some studies evaluated the efficacy of hand scalers, sonic and ultrasonic scalers in calculus removal from the furcation of multi-rooted teeth. It was found that sonic and ultrasonic scalers allow more efficient cleaning of furcation as compared to hand scalers 23, 24. Comparison of calculus removal with sonic (Titan-S sonic scaler) and ultrasonic scaler (Dentsply Cavitron ultrasonic scaler) was done on extracted teeth in one study. Using scanning electron microscopy, the results indicated that the Titan-S sonic scaler was as effective at calculus removal as the Dentsply Cavitron ultrasonic scaler and surface roughness was found to be less with sonic scaler 25.
Removal of endotoxins from cementum surface:
Initially, it was believed that complete cementum removal was necessary in order to remove the disease-causing agents, but later on, research showed that extensive removal of cementum is not necessary to render the root free of bacterial endotoxins 26. The objective of scaling and root planing is the complete removal of plaque, calculus and the endotoxin adherent to the root surface. It is now clear that cementum removal is unnecessary. Various studies have compared the removal of endotoxin from the root surface by using hand instruments 27, 28 and ultrasonic devices 27-29. Most of them have found …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Post scaling and root planing evaluation:
Immediately after scaling and root planing, root surface smoothness can be evaluated, but soft tissue evaluation should not be done immediately after scaling. It has been shown that the re-epithelialization of the injured area during scaling takes place within 1 to 2 weeks 30, 31. Junctional epithelium can be expected to take approximately one week to heal following the debridement whereas underlying connective tissue can take 4-6 weeks 32-34. During this period of healing gingival bleeding can be expected during probing. If the patient is maintaining a good oral hygiene and regularly following advised brushing technique, complete healing takes place during this time period, after which patient can be re-evaluated.
VectorTM system
The VectorTM system (Dϋrr Dental, Bietigheim-Bissingen, Germany) is a newly developed ultrasonic system, with an oscillation frequency of 25 kHz. This device generates ultrasonic vibrations which are converted by a resonating ring in such a way that horizontal oscillations are deflected vertically because of which the tip of the scaler moves parallel to the root surface. Hence, damage to the root surface is minimal. This system is recommended for use in conjunction with irrigation fluids containing hydroxylapatite or silicon carbide 35. These spraying agents disrupt the plaque during the scaling procedure to increase the efficiency and achieve better clinical results.

The hydrodynamic forces such as cavitation or acoustic microstreaming are supposed to be responsible for cleaning of tooth surface rather than chipping action of the instrument tip 9. The major advantage of this system is, patient comfort. By avoiding vibrations applied horizontally to the root surface, treatment with this system has been shown to be less painful than treatment with conventional systems 36.
Studies have compared the VectorTM system with the conventional ultrasonic scalers and hand instrumentation for its efficacy. One study demonstrated complete removal of calculus from the root surface, however, the efficiency was dependent on the fluid used 37. In another study, it was shown that the calculus removal efficiency of the Vector system was lower than that of hand instrumentation and the conventional ultrasonic system, however; the root surfaces scaled by the Vector system were less traumatized and it was emphasized that Vector system was more promising to use in a regular maintenance therapy to avoid the high loss of cementum and dentine 38. One more study done on this system demonstrated the root surface roughness comparable to hand instruments 39.
Ultrasonic scalers associated hazards
Aerosol and splatter:
Centers for Disease Control and Prevention recommends that all sources of blood-contaminated splatter and aerosols should be minimized during dental treatment. One of the major sources of potential aerosol and splatter contamination in the dental setting is the ultrasonic scaler. Micik and colleagues (1969) 40 have defined dental aerosols and splatter. Aerosols have been described as particles smaller than 50 μm whereas particles larger than 50µm have been described as splatter 40. It has been demonstrated that these particles behave in a ballistic manner, i.e., after ejection from the operating site they arch in a trajectory similar to that of a bullet until they contact a surface or fall on the floor 41.
There are two types of infectious aerosols: dust born and droplet nuclei. The dust born aerosols are larger in diameter and they can be easily removed from the air by sedimentation or filtration. They are less likely to cause infection. On the other hand, the droplet aerosols are smaller in size and settle out of the air slowly. Being smaller and lighter, these droplet nuclei particles can remain in the environment for a longer period of time. These can easily spread in the dental operatory with air currents and can contaminate open surfaces and equipment. So, droplet aerosols pose a greater risk to the patients and health care providers as compared to dust born aerosols. Viral particles, such as Human immunodeficiency virus and Hepatitis B virus are easily carried by these particles.
According to the American Dental Association (ADA), aerosol contamination is to be minimized: 1) by the use of a rubber dam whenever possible; 2) by the use of a high-volume evacuator (HVE); and 3) by proper patient positioning 42. It has been shown in one study that after ultrasonic scaling, bacteria could be recovered 6 inches from the mouth of the patient and that the number of colony forming units was significantly reduced when an aerosol reduction device was used during scaling 43.
Adverse effects of noise:
The noise exposure from ultrasonic scalers commonly produces hearing loss over a long period of time and can temporarily alter patient’s hearing 44. The frequency at which ultrasonic scalers work range from 20,000 to 50,000 vibrations per second with a 68 to 75 average decibel range of noise level 45, 46. One study has proposed that ultrasonic scaling units produce high-frequency vibrations, which have the potential to cause occupational hearing loss 47. A study demonstrated levels of annoyance and discomfort from high-frequency noise produced by ultrasonic cleaners ranging from 72 to 96 decibels 48.
Thermal hazards:
Excessive heat may be produced during scaling which is mainly due to functional heating due to contact between scaler and tooth and acoustic energy absorption of ultrasound transmitted into the tooth. It has been shown that absorption of acoustic energy by the tooth surface can result in the elevation of tooth temperature, causing heat injury 49. It has been shown that an increase in temperature above 11°C can invariably damages the pulp and a 17°C increase can cause pulp death 50. Performing ultrasonic scaling without irrigation leads to increase in temperature, and may completely damage the pulp tissue. The coolant flow rate during scaling should be at least 20-30 ml/min 51.
Proprioceptive dysfunction:
Proprioceptive dysfunction can often be caused by noise exposure. The most common reasons for proprioceptive dysfunction include vestibular dysfunction and peripheral neuropathy. Proprioceptive dysfunction may, in turn, can affect other sensory organs, including the sense of touch 52. Nystagmus or involuntary movement of the eyeball is a common example of vestibular dysfunction. In dental practitioners, peripheral neuropathies can cause difficulties in proprioception. Persons with peripheral neuropathies have little or no tactile sensitivity and are prone to self-injury because of their inability to feel stimuli. It may impair the ability of oral health provider to evaluate the root surface after therapeutic scaling.
Tactile sensitivity:
Tactile sensitivity is the ability to distinguish relative degrees of tooth surface roughness or smoothness through the sense of touch and proprioception. Tactile sensitivity may be impaired because of musculoskeletal and nerve disorders associated with cumulative trauma, repetitive tasks, and high-frequency vibrations. When exposed to vibrations, tactile sensitivity may be one of the first physiological components to be affected. One Study has reported reduced tactile …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Affect on pacemakers:
Cardiac pacemakers have been designed to regulate the rhythm of the heart. There are basically two types of cardiac pacemakers: competitive (fixed rate type) and noncompetitive (demand type). The competitive pacemakers discharge at a fixed rate while the non-competitive pacemakers discharge if the rate becomes irregular. Presently, noncompetitive pacemakers are almost exclusively used. The electromagnetic field produced by the magnetostrictive ultrasonic scalers during scaling may interfere with the pacemaker discharge rate, which may cause a serious life-threatening condition 55. Initial pacemakers were more susceptible to the external electromagnetic field as their circuit was not shielded. Current pacemakers are relatively immune to electromagnetic interference because the circuitry is shielded inside a hermetically sealed titanium or stainless steel case that often has an additional insulative coating. In addition, increased use of bipolar leads has also decreased the susceptibility of pacing systems to electromagnetic interference. However, while operating on a patient with cardiac pacemaker, the guidelines provided by the manufacturing company of the pacemaker should be thoroughly studied by the operating dentist.
How to reduce aerosol contamination
Although, it is impossible to determine the exact infection risk represented by aerosols but appropriate measures can definitely reduce the risk of infection. The use of personal barrier protection such as masks, gloves, and eye protection will eliminate much of the danger inherent in splatter droplets arising from the operative site. It has been shown that true aerosol particles (particles less than 50 μm in diameter) have the potential to enter the respiratory tract through leaks in masks 56. Another effective way of reducing overall bacterial counts produced during dental procedures is the use of a pre-procedural rinse. Research has demonstrated that the use of chlorhexidine or essential oil-containing mouthwash for one minute before a dental procedure can significantly reduce the bacterial count in the air of the operatory 57.
Use of high-volume evacuator (HVE) is also a very useful way to reduce aerosol contamination. HVE removes a large volume of air within a short period. Evacuators which pull a high vacuum, but do not remove a large volume of air are not considered an HVE. HVE used by dentists usually have an opening of 8 mm or more and evacuates up to 100 cubic feet of air per minute. It has been shown that the use of HVE can reduce the contamination arising from the operative site by …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Conclusion
In the above discussion, the power-driven scalers were discussed in detail. There are many advantages of using powered scaling devices which include reduced time, reduced mechanical effort and reduced tooth structure loss. Along with this, hazards associated with the use of these devices include aerosol contamination, proprioceptive dysfunction, noise associated problems, heat associated hazards, adverse effects on tactile sensitivity and adverse effects on electronic devices like cardiac pacemakers. Preventive measures should be taken to reduce the risk of spread of infection during the use of these devices.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.