Introduction
One of the major challenges faced by dental specialists today is the assessment and management of patients with increasingly complex medical conditions. These medical conditions can alter both, the course of the oral disease and the therapy provided. Therefore, it is important for a clinician to identify patient’s medical status to formulate a proper treatment plan. The life expectancy has increased dramatically in past decades. Geriatric patients are much more likely to have a complex medical history and the use of multiple medications. The common medical conditions encountered by the periodontists in daily practice include cardiac diseases, pulmonary diseases, hypertension, diabetes, bleeding disorders, renal disorders, pregnant patients and patients undergoing radiation therapy.
Importance of history taking
A thorough history taking is of prime importance when starting with the management of a patient. Many times patients cannot correlate their medical condition with their dental problems. So, it becomes important to ask the patient-relevant questions to obtain an accurate medical history. A well-designed questionnaire can be designed to obtain a proper medical history of the patient. The analysis of information collected achieves three important objectives: enables the monitoring of medical conditions and the evaluation of underlying systemic conditions of which the patient may or may not be aware; provides a basis for …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Cardiovascular diseases
Cardiovascular diseases (CVD) is a broad term used to categorize any abnormal condition characterized by dysfunction of the heart and blood vessels. There are a number of cardiac conditions which may be present in a patient seeking periodontal treatment.
Hypertension
Hypertension or high blood pressure is a common cardiovascular disease. It is a major risk factor for ischemic and hemorrhagic stroke, myocardial infarction, heart failure, chronic kidney disease, cognitive decline and premature death. The risk associated with increasing blood pressure is continuous, with each 2 mm Hg rise in systolic blood pressure associated with a 7% increased risk of mortality from ischemic heart disease and a 10% increased risk of mortality from stroke. Hypertension can be classified as primary or secondary hypertension.
Primary or Essential Hypertension (without an organic cause):
Primary hypertension is the term used for medium to high blood pressure for a long time (chronic) without a known cause, which is a very common form of hypertension, comprising about 90-95% of all patients with hypertension 3.
Secondary Hypertension:
Hypertension with a well established organic cause which includes the following:
Renal (parenchymal or renal vascular): Chronic pyelonephritis, acute and chronic glomerulonephritis, polycystic kidney disease, renal vascular stenosis or renal infarction, other severe kidney diseases (arteriolar nephrosclerosis), renin-secreting tumors;
Endocrine: Oral contraceptives, adrenal hyperfunction (Cushing’s syndrome, primary aldosteronism, congenital or hereditary adrenogenital syndrome), pheochromocytoma, myxedema, acromegaly, thyroid and parathyroid hyperfunction;
Neurological: Psychogenic “diencephalic syndrome,” familiar dysautonomia (Riley-Day), polyneuritis (acute porphyria, lead poisoning), increased intracranial pressure;
Others: Coarctation of the aorta, increased intravascular volume (transfusion excessive polycythemia vera), polyarteritis, hypercalcemia, drugs (corticosteroids, cyclosporine), sleep apnea, pregnancy toxemia, acute intermittent porphyria.
The Seventh report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure gave a classification of blood pressure for adults aged ≥18 years 4. According to this classification, normal blood pressure is defined as levels <120/80 mm Hg. Systolic blood pressure of 120-139 mm Hg or diastolic blood pressure 80-89 mm Hg is classified as prehypertension. Hypertension is defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg. Hypertension is divided into two stages.
Classification of blood pressure.
Blood pressure classification Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg)
Normal <120 And <80
Prehypertension 120-139 or 80-89
Stage 1 hypertension 140-159 or 90-99
Stage 1 hypertension ≥160 or ≥100
- Stage 1 includes patients with systolic blood pressure 140-159 mm Hg or diastolic blood pressure 90-99 mm Hg.
- Stage 2 includes patients with systolic blood pressure ≥160 mm Hg or diastolic blood pressure ≥100 mm Hg.
A more elaborate classification of blood pressure is provided by the European Society of Hypertension and the European Society of Cardiology 5.
Classification of blood pressure for adults.
Category Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg)
Optimal <120 <80
Normal 120-129 80-84
High normal 130-139 85-89
Grade 1 hypertension
(mild)140-159 90-99
Grade 2 hypertension
(moderate)160-179 100-109
Grade 3 hypertension
(severe)≥180 ≥100
Isolated systolic
hypertension≥140 <90
The diagnosis of hypertension in adults is made when the average of two or more diastolic blood pressure measurements on at least two subsequent visits is ≥90 mm Hg, or when the average of multiple systolic blood pressure readings on two or more subsequent visits is ≥140 mm Hg.
Management of a hypertensive patient
Once the patient is an established hypertensive, proper precautions should be taken to prevent any complication during periodontal treatment. Before starting any treatment, blood pressure has to be checked. Accurate measurement of blood pressure is important to avoid overdiagnosis or underdiagnosis, as well as overtreatment or undertreatment, of hypertension. The patient should be allowed to sit for 3-5 minutes before taking blood pressure measurements. At least two blood pressure measurements should be taken in the sitting position, spaced 1-2 minutes apart and additional measurements if the first two are quite different. The average of the …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..
There is no change in the treatment plan if the systolic blood pressure is <140 mm Hg and diastolic blood pressure is <90 mm Hg. If systolic blood pressure is 140-159 mm Hg and diastolic blood pressure is 90-99 mm Hg, the patient is informed about the findings and is referred to the physician. If systolic blood pressure is 160-179 mm Hg and diastolic blood pressure is 100-109 mm Hg, only selective treatment is done, including routine examination, oral prophylaxis, and restorative procedures. Surgical procedures should be avoided. In the case of severe hypertension with systolic blood pressure ≥ 180 mm Hg and diastolic blood pressure ≥ 110 mm Hg, only emergency treatment is done to alleviate the pain and immediate referral to the physician is recommended.
If the patient is already on antihypertensive drugs, the local anesthetic (LA) agent may interact with these drugs. Interaction of LA with non-selective β-blockers may increase LA toxicity 6. Stress is another important factor which may complicate the dental treatment in hypertensive patients. Patients with cardiovascular diseases have a high risk of complications due to endogenous catecholamines (adrenaline and noradrenaline) released due to pain and stress. These may dramatically increase blood pressure and cardiac output. Various steps that may be taken to minimize stress are,
- Shorter appointments.
- Good night’s sleep before the appointment.
- Avoiding caffeine before the appointment.
- Eating a regular meal before the appointment.
- Pre-anesthetic medications as needed.
- Make sure that daily dose of anti-hypertesive medication has been taken by the patient.
- Sudden changes in body position should be avoided, as they can cause orthostatic hypotension as a side effect of the blood pressure-lowering drugs.
Pain during treatment may also result in the release of endogenous catecholamines. During treatment, pain should be minimized so that the release of endogenous catecholamines is reduced. It must be noted that epinephrine prolongs the action of LA due to its vasoconstriction effect, but LA with vasoconstrictor should be avoided or used in low doses in patients taking non-selective β-blockers or in patients with uncontrolled hypertension. The recommended dose of epinephrine in a patient with cardiac risk is 0.04 mg, which is equal to that containing about two cartridges of LA with 1 : 100000 epinephrine or 4 cartridges with 1 : 200000 epinephrine 7. It is better to measure the blood pressure after administering LA in patients with …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..
Management of hypertensive crisis:
The term hypertensive crisis is defined as an elevation of the blood pressure to a degree which is potentially life-threatening and that requires immediate management. It is important to emphasize that the clinical distinction between hypertensive emergencies (crises) and hypertensive urgencies depends on the presence of acute target organ damage, rather than the absolute level of blood pressure. Hypertensive emergencies are those which involve end-organ damage such as hypertensive encephalopathy, acute left ventricular failure or pulmonary edema, acute myocardial ischemia, eclampsia, acute renal failure, dissecting aortic aneurysm or symptomatic microangiopathic hemolytic anemia. On the other hand, in hypertensive urgencies, the increase in blood pressure (usually blood pressure greater than 220/120 mmHg) is not associated with any evidence of acute end-organ damage. In female patients during pregnancy, around 10% of them show hypertension and approximately 1-2% undergo a hypertensive crisis. In pregnancy, systolic blood pressure > 160 mm Hg or diastolic blood pressure >110 mm Hg is considered as hypertensive crisis 8.
In the recent past, the most popular agent for the treatment of hypertensive urgencies was short-acting nifedipine, given either sublingually or orally 9. Several severe side effects, however, have been reported with its use 10. These include loss of consciousness, hemiparesis, ECG changes, myocardial infarction and complete heart block 10-12. Other agents with a relatively fast onset of action which can be used for the management of hypertensive urgencies include captopril (angiotensin-converting enzyme (ACE) inhibitor), esmolol (ultra-short-acting, cardioselective, β-adrenergic blocking agent), nitroprusside (vasodilator), labetalol (α- and β-adrenergic blocker), atenolol (β-adrenergic blocker), and clonidine (central α-2 agonists) 13.
Ischemic heart diseases
Angina pectoris:
Ischemic Heart Disease, also known as Coronary Artery Disease (CAD), is a condition that affects the supply of blood to the heart. The blood vessels are narrowed or blocked due to the deposition of cholesterol on their walls. This reduces the supply of oxygen and nutrients to the heart muscles, which is essential for proper functioning of the heart. This may eventually result in a portion of the heart being suddenly deprived of its blood supply leading to the death of that area of heart tissue, resulting in a heart attack.
An important indicator of CAD is angina pectoris, defined as a syndrome of substernal chest discomfort, with a characteristic quality and duration that is provoked by exertion or emotional stress, and is relieved by rest or the administration of nitroglycerin. In angina the myocardial oxygen demand exceeds the supply, resulting in temporary myocardial ischemia. Angina pectoris may be of two types: stable and unstable. In the case of stable angina, the patient has pain, lasting 5-15 minutes, which is relieved by administration of nitroglycerin. It usually has a trigger, such as physical exercise or exertion, anxiety, or emotional stress, cold temperatures, or heavy meals. In unstable angina, the patient has pain lasting longer …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..
Acute myocardial infarction (AMI):
Acute myocardial infarction results due to physical disruption of an atherosclerotic plaque with subsequent formation of an occluding thrombus, coronary occlusion causing a reduction in coronary blood flow. This results in ischemia of heart muscles which are supplied by the occluded artery. Myocardial necrosis caused by complete coronary artery occlusion begin to develop after 15-30 min of severe ischemia (no forward or collateral flow) and progresses from the subendocardium to the subepicardium in a time-dependent fashion. The condition is characterized by acute, sudden onset and intense pain, of an oppressive nature, located in the retrosternal or precordial region, and can radiate to the arms, neck, back, jaw, palate or tongue. Other clinical features that may be seen are intense perspiration, nausea, vomiting, dyspnea and imminent death sensation, though it can also manifest as sudden loss of consciousness, mental confusion or weakness. Another form of AMI may be silent infarctions. Silent infarctions are characterized by an absence of pain, and are more common in elderly individuals, in women and in diabetic patients 14, 15.
AMI can be confirmed by different perspectives related to electrocardiographic (ECG), biochemical, and pathological characteristics. The present guidelines pertain to patients presenting with ischemic symptoms and persistent ST-segment elevation on the ECG. The acute myocardial infarction if not treated well in time results in congestive heart failure and death of the patient.
Congestive heart failure:
Congestive heart failure can be defined as the incapacity of the heart to function properly, pumping insufficient blood towards the tissues and leading to fluid accumulation within the lungs, liver, and peripheral tissues. The congestive heart failure is the end result of ischemic heart diseases or arterial hypertension. Heart failure may be acute or chronic in nature. Acute heart failure is triggered by cardiotoxic drugs or coronary occlusion episodes. The most common causes for this are …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..
Pathophysiology of ischemic heart disease:
Although, many theories exist regarding the development of atherosclerosis, but the response-to-injury hypothesis is currently the most popular, with the initial “injury” occurring at the level of vascular endothelium 17. According to this hypothesis, the initial endothelial damage is caused by hemodynamic forces. These forces are more common at the arterial branches and bifurcations where atherosclerotic plaques usually develop. Endothelial injury is followed by the adherence of platelets, release of platelet-derived growth factor, migration of monocytes into the intima, and migration and proliferation of smooth muscle cells from the media. These result in the production of an atherosclerotic plaque. Repeated episodes of injury result in progressive narrowing of the vascular lumen by a vicious cycle of flow disturbance, endothelial injury, and plaque growth 18.
Periodontal treatment of patients with ischemic heart disease
Patients with ischemic heart disease may be stable or unstable. In an unstable patient only elective dental treatment is indicated with medical consultation. Emergency dental care for the unstable patient should be conservative, principally consisting of the use of analgesics and antibiotics. In stable patients, dental treatment can be carried out without mandatory medical consultation. Nitroglycerine is given to patients to treat acute anginal attacks. They should be asked to bring the drug with them during their dental appointments. Use of vasoconstrictor should be limited, taking care not to exceed 0.04 mg of adrenaline (2 carpules containing 1.8 ml of anesthetic with adrenaline 1: 100,000). The technique of administration of local anesthesia should be accurate, taking care not to inject the solution into a blood vessel. If more local anesthesia has to be administered, it should be provided without a vasoconstrictor 19.
To reduce anxiety, premedication can be administered to lessen anxiety and stress (5-10 mg of diazepam the night before and 1-2 hours before treatment). Inhalatory sedation in the form of nitrous oxide / oxygen has also been recommended by some authors 20. To minimize stress during treatment, the same steps are taken as explained for the hypertensive patients. This reduces endogenous catecholamine secretion, thus preventing complications related to vasoconstriction. If the patient is taking anticoagulants, the international normalized ratio (INR) should be determined prior to any surgical procedure. If the INR is < 2.5, there is no need to …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..
Patients who had an acute myocardial infarction episode recently, are at a greater risk of developing another infarction episode or severe arrhythmias. It has been shown that around 70% of all recurrences take place in the first month after the initial vascular event 22. In such cases, only emergency treatment should be done aimed at affording pain relief. Extractions, drainage of abscesses and pulpectomies are preferably carried out in the hospital setting. The time period following a myocardial infarction after which dental treatment can be done safely has not been well established.
However, many authors consider 4-6 weeks after infarction to be a prudent period 14. In the case of recent acute myocardial infarction episode, it is a must, to consult the physician to know the type and severity of the cardiac problem, the complications that may arise during treatment and the medicines the patient is taking. As already stated, if the patient is taking nitrates, he/she should bring them to the dental clinic on each visit. The steps to control and minimize stress are same as described before.
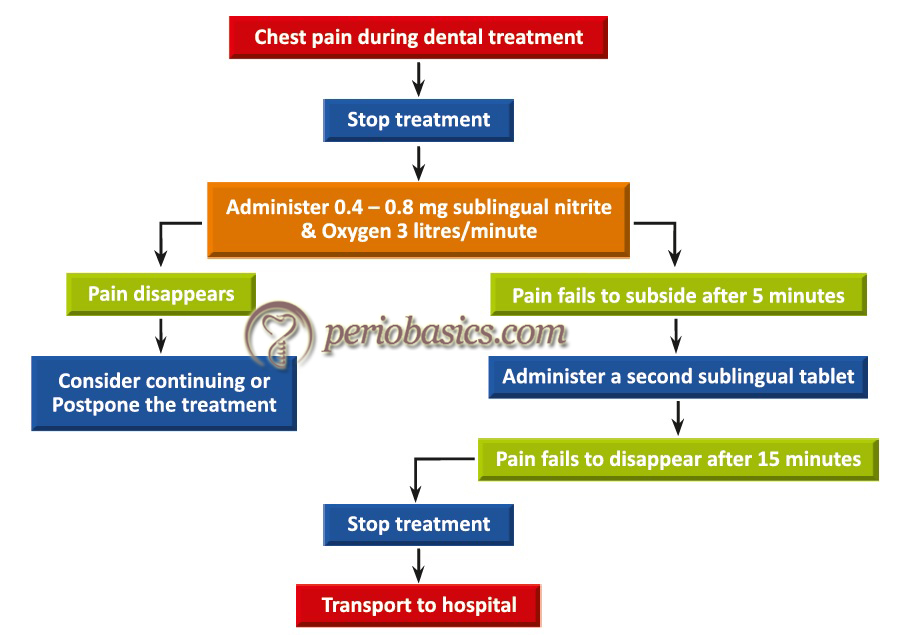
During the treatment, if the patient develops chest pain administration of nitroglycerine (0.4-0.8 mg) is recommended. Nasal oxygen supply, 3 liters/minute should be immediately established. If the pain subsides and the patient improves, the treatment can be continued otherwise the procedure is postponed. If the pain does not subside within next five minutes, another sublingual tablet should be administered. But, if the pain does not subside even after 15 minutes of onset, myocardial infarction has to be suspected and the patient must be transferred to a hospital immediately.
Infective endocarditis (IE)
IE is an infection of the inner lining of the heart and heart valves. The etiology of more than 85% of all IE cases is bacteria, most often Staphylococci, Streptococci, and Enterococci 23. Other bacteria implicated for IE belong to HACEK group of microorganisms (Haemophilus parainfluenza, H. aphrophilus, H. paraphrophilus, H. influenzae, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella kingae, and K. denitrificans). Fungi have also been isolated from the IE lesions. IE has been classified into acute and subacute types, according to the natural history of the disease. Recently, as the number of cases with valve replacement surgery is increasing, the number of endocarditis cases associated with the prosthetic valves has increased. Therefore, these diseases are also classified into “prosthetic valve endocarditis” and “native valve endocarditis”.
Pathogenesis of IE:
Normally, the cardiac valves are resistant to colonization and infection by circulating bacteria. But, if there is any mechanical disruption of the endothelium, it results in the exposure of underlying extracellular matrix proteins, production of tissue factor, and the deposition of fibrin and platelets as a normal healing process. Such nonbacterial thrombotic endocarditis (NBTE) facilitates bacterial adherence and infection. There are many reasons for the mechanical damage to the cardiac valves including, turbulent blood flow, electrodes or catheters, inflammation (as in rheumatic carditis), or degenerative changes in elderly individuals.
The mechanical damage leads to an inflammatory response which results in the formation of micro-ulcers and micro-thrombi. The inflammation results in the expression of integrins of the β1 family (very late antigen) by the endothelial cells. These bind to the circulating fibronectin. S. aureus and some other IE pathogens carry fibronectin-binding proteins on their surface, facilitating their colonization in that area. After adhering, S. aureus triggers their active internalization into valve endothelial cells, where they can either persist and escape host defenses and antibiotics, or multiply and spread to distant organs 24.
The primary bacteria …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Antibiotic prophylaxis to prevent infective endocarditis:
The bloodstream is sterile under normal conditions. The introduction of bacteria into the bloodstream is necessary for an intracardiac infection to occur. Any dental treatment which involves bleeding may result in bacteremia. It must be noted that not only the surgical procedures but non-surgical procedures have also been reported to cause bacteriemia. These include the administration of local anesthesia 26, periodontal probing 27, dental prophylaxis 28, scaling and root planing 29, and even daily tooth brushing 30 and flossing 31.
To reduce the risk of IE following dental procedures, prophylactic measures have been developed. The principal preventive measure recommended is the use of prophylactic antibiotics before certain dental procedures in patients identified as at risk. The American Heart Association first recommended prophylaxis regimen which was issued in 1955 but changes have done and most current recommendations were issued in 2007 32. Following table describes the American Heart Association guidelines for the identification of patients who may require prophylaxis for infective endocarditis before dental procedures,
| American Heart Association guidelines for the identification of patients who may require prophylaxis for infective endocarditis before dental procedures. |
|---|
| • Prosthetic cardiac valve. • Previous infective endocarditis. • Congenital heart disease (CHD), if 1 of the 3 conditions listed below is present: 1. Unrepaired cyanotic CHD, including palliative shunts and conduits. 2. Completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 months after the procedure. 3. Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device (which inhibit endothelialization). • Cardiac transplantation recipients who develop cardiac valvulopathy. |
Dental procedures for which antibiotic prophylaxis is recommended:
According to the American Heart Association (2007), follow-ing dental procedures require antibiotic prophylaxis,
Manipulation of gingival, periodontal and periapical tissues; incision of mucosa including:
- Surgery.
- Periodontal procedures.
- Endodontic instrumentation beyond the apex or apical surgery.
- Subgingival placement of antibiotic fibers or strips.
- Initial placement of orthodontic bands, but not brackets.
- Intraligamentary local anesthetic injections.
- Prophylactic cleaning of teeth or implants where bleeding is anticipated.
Excluding: Local anesthetic agent administration (unless through the site of infection).
Regimens for infective endocarditis prophylaxis:
The American Heart Association (2007) 32 has specified the antibiotic regimen for prophylaxis of infective endocarditis. The following table describes the AHA regimens for infective endocarditis prophylaxis.

Periodontal treatment of an infective endocarditis patient:
As bacteremia is associated with the development of infective endocarditis, the first step during periodontal treatment is to define a susceptible patient. The guidelines provided by American Heart Association 32 describe high-risk patients who are susceptible to the development of infective endocarditis. A history of the medical illness can indicate the risk of development of IE, but if required patient’s physician should be consulted to know the exact status of the disease. The patient should be given oral hygiene instructions to reduce bacterial load in the oral cavity. The patient should be …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..
If the patient is taking oral penicillin for prevention of rheumatic fever, penicillin-resistant α-hemolytic Streptococci may be found in the oral cavity. Therefore, the alternate regimen can be followed. If the patient is already taking oral penicillin for periodontal treatment, the IE prophylaxis regimen is changed. Following steps should be followed during periodontal treatment of an IE patient,
- All the periodontal treatments, including periodontal probing, should be carried out under antibiotic prophylaxis.
- Chlorhexidine mouth rinses are recommended before all periodontal treatments because they significantly reduce the presence of bacteria on mucosal surfaces 34.
- The number of appointments should be reduced by clubbing different treatments according to patients need and tolerability 35. It reduces the chances of developing resistant bacteria. Minimum of one week (preferably 10-14 days) gap should be kept between the two appointments, but if it is less than one week, the alternate antibiotic regimen should be selected (Table 32.5). Using the same antibiotic between dental hygiene appointments that are scheduled within a 9-day period increases the risk of resistance and may reduce the efficacy of the drug.
- It should be remembered that if the patient is taking antibiotic following periodontal treatment, the standard prophylactic dose is still needed before starting the next periodontal treatment during next appointment. Reason being, the regular antibiotic dosage is not adequate to prevent the development of IE. For example, if a patient has been taking amoxicillin 250 mg three times a day for 10 days after periodontal surgery and he/she is scheduled for next treatment after 7 days following surgery, he/she should be given full 2 gm dose of amoxicillin before starting the treatment or alternative drug regimen should be chosen such as azithromycin or clindamycin.
- During the maintenance phase, the oral hygiene status of the patient should be re-evaluated with an emphasis on oral hygiene reinforcement.
Antibiotic prophylaxis recommendations for adults at risk for IE who require multiple dental hygiene appointments within a 9-day period
| Appointment | Antibiotic |
|---|---|
| First | Amoxicillin 2 gm |
| Second (2-4 days later) | Macrolide (clarithromycin or azithromycin) 500 mg |
| Third (2-4 days later) | Clindamycin 600 mg |
| Fourth (2-4 days later) | Amoxicillin or cephalexin 2.0 gm |
| Fifth (2-4 days later) | Macrolide |
Patients with cardiac pacemakers and cardioverter-defibrillators
Different types of cardiovascular implantable electronic devices, chiefly implantable cardiac pacemakers and implantable cardioverter- defibrillators, are used to treat a variety of electrical cardiac defects, including bradyarrhythmia, ventricular tachycardia, and fibrillation; they are also used in patients with complete heart block 36, 37. Use of such devices has significantly reduced mortality rates among patients with a history of life-threatening ventricular arrhythmia, and they are becoming more commonplace in the general population. A cardiac pacemaker is a device that regulates heartbeat. It is a small device sealed in a metal case consisting of a pulse generator, which produces an electrical impulse that is sent directly to the cardiac muscles via plastic-coated wires, and a long-lasting battery 38. A pacemaker is usually implanted under the skin in the chest wall. The different types of implantable pacemakers are as follows:
- Fixed-rate pacemaker: This type of pacemakers is intended for patients with permanent heart blocks.
- Demand pacemaker: These pacemakers have gradually replaced the fixed-rate pacemakers because they avoid the competition between the heart’s natural rhythm and the pacemaker rhythm.
- R wave triggered pacemaker: This type of pacemaker is meant for patients who generally have heart block with occasional heart sinus rhythm.
- Ventricular inhibited or R-wave blocked pacemaker: This type of pacemaker is meant for patients who generally have sinus rhythm with occasional heart block.
- Atrial triggered pacemaker: This is a type of pacemaker that detects the atrial depolarization and starts the pulse forming circuits after a delay so that the impulse to the ventricles is delivered after a suitable PR interval.
- Dual-chamber pacemaker: These devices are commonly capable of treating the majority of those patients who suffer from diseases of the sino-atrial node by providing atrial stimulation whenever needed.
Implantable cardioverter-defibrillators are similar to pacemakers, in that both devices are designed to monitor the heart rate continuously. When ventricular tachycardia or fibrillation is detected, the cardioverter-defibrillator delivers a precisely calibrated shock to stop the abnormal electrical activity and restore the normal heart rate 36.
Pacemakers and other implanted cardiac devices are sensitive to strong electromagnetic signals that may temporarily interfere with function. The initially designed pacemakers and other implanted cardiac devices were not shielded and ultrasonic dental equipments were implicated in electrical interference with their normal functioning. Miller et al. (1998) 39 used telemetry for in vitro evaluation of the Medtronics Thera 7942 dual-chamber bipolar pacemaker and the Minix 8340 single-chamber unipolar pacemaker. The results demonstrated that both atrial and ventricular pacing, particularly in the unipolar pacemaker, was inhibited by electromagnetic interference produced by the magnetostrictive ultrasonic scaler. In another study, Trenter and Walmsley (2003) 40 reported that magnetostrictive scalers may interfere with the operation of pacemakers, but that piezo-electric ultrasonic scalers did not affect pacemaker function. Presently, most of the devices are designed with safeguards that include electronic filters or shields that insulate the device in the presence of electromagnetic interference.
Management of patients with pacemakers and cardioverter-defibrillators:
All the patients who have been implanted with pacemakers and cardioverter-defibrillators should be asked to bring the details about the device. The manufacturer of the device, model number, serial number, date of implantation and mode of operation of the device should be documented in the patient’s record. Based on the current evidence, it is recommended that use of magnetostrictive ultrasonic equipments should be avoided on or near the individuals with implantable cardiac pacemakers or cardioverter-defibrillators 38. Electrosurgical units also cause marked interference with the functioning of these devices. The piezoelectric ultrasonic scaler devices can be used safely in these patients 38, 40. Care should be …….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…….. Contents available in the book…..
Conclusion
There are many patients who have cardiovascular problems, seeking periodontal treatment. In-depth knowledge of these conditions and their management is essential for periodontists so that these patients are adequately treated without causing any complications. In the upcoming articles, we shall read about other medical conditions that need special attention while performing dental treatments.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.