Introduction
Due to improvement in the health care facilities the population of elderly individuals in increasing throughout the world. The oral health-related problems in geriatric patients are different from those seen in younger individuals. One of the most important criteria determining the oral and periodontal health in elderly individuals is how they have been taking care of their oral health throughout their lifetime. To understand the oral health-related problems, first we need to understand the concept of complete oral health. Oral health implies a state that is stable, relatively disease-free and comfortable and that permits adequate functioning for mastication, swallowing and speech. Any deviation from adequate function or esthetics can be considered as a part of oral health-related problem.
In elderly individuals, these problems vary from presence of periodontal disease including presence of inflammation with or without active periodontal destruction, decayed teeth and ill-fitting dentures or lack of dentures. In the following discussion, we shall discuss in detail the oral problems in geriatric patients and their management.
Physiological changes in the oral and peri-oral structures in elderly individuals
Hard tissue changes
Alveolar bone:
The alveolar bone is a very dynamic tissue. Its formation starts with the eruption of teeth and with increasing age, it is continuously remodeled to best withstand the occlusal forces. It has been observed that rate of remodeling of alveolar bone is greater than bones in other part of the body 1. With increasing age, the rate of remodeling of alveolar bone decreases as observed in other parts of body. It has been observed that approximately 1% of bone mass is lost per year in both men and women, after the age 35 to 40 years 1. Thus, in geriatric patients, there is a generalized decline in the ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Teeth:
Teeth differ from other calcified tissues in body in that they have a limited reparative or regenerative capacity. Furthermore, the blood supply and the nerve supply of the teeth become less active with increasing age. It has been observed that on an average, the vitality of tooth lasts around 70 years 3. The most common tooth-related finding with ageing is attrition. There is a natural wear of teeth due to masticatory function. In patients with bruxism, the attrition may be so severe that it may result in pulpal involvement. To compensate for the occlusal wear, there is a continuous eruption of teeth throughout the lifetime of an individual 4.
Know More…
Differences between attrition, abrasion, erosion and abfraction:
Attrition:
It refers to the loss of tooth structure by mechanical forces from opposing teeth. It is limited to the contacting surfaces of the teeth. Bruxism is the most common cause of attrition.
Abrasion:
It is the loss of tooth structure due to mechanical action of a foreign element, such as a hard bristle toothbrush or a lip piercing. The abrasion lesion is typically narrow in relation to depth.
Erosion:
It is the loss of tooth structure due to chemicals. Chemicals involved in dental erosion are usually acidic, such as carbonated beverages, citrus fruits, tart candy, or stomach acid (bulimia; gastric reflux). Clinically, areas of erosion are sharply defined with saucer shaped tooth defects. These are usually present in the facial and cervical areas.
Abfraction:
It refers to the pathological loss of enamel and dentine due to occlusal stresses. It usually results from occlusal forces which cause the tooth to flex, resulting in small enamel flecks to break off at the cervical areas.
Temporomandibular joint (TMJ):
The TMJ is a complex joint which facilitates a variety of mandibular movements during its various functions. This joint is subjected to continuous remodeling throughout the lifetime of an individual. It has been reported that the TMJ related problems are more common in females than in males 5. The most common signs and symptoms associated with TMJ disorders include pain during jaw movement, clicking sound during jaw opening, deviation of the jaw during mouth opening and limitation of jaw opening.
Soft tissue changes
Oral mucosa:
With aging many changes are observed in the oral mucosa. These changes include thinning of the oral epithelium with oral mucosa becoming less elastic, less vascular and less firmly attached to the underlying connective tissue and bone. Because of these reasons, the oral mucosa becomes more susceptible to injury from mild stresses 3, 6. Along with this, there is reduction in connective tissue and subcutaneous fat and increased linkage of collagen molecules. The symptoms associated with these changes include burning or pain sensation in tongue, palate, or oral mucosa 7. However, these findings should be interpreted with caution when diagnosing the patients, to differentiate between physiological and pathological changes in the oral cavity 8.
Periodontium:
A detailed description of age-related changes in the components of periodontium has been discussed in “Effects of aging on the periodontium”.
Oral musculature:
In general, there is a reduction in the number and size of muscle fibers in muscles throughout the body with ageing and peri-oral muscles are no exception to it. With increasing age there is a reduction in the muscle tone and muscle performance 9, 10. There is a reduction in the muscle mass and fatty tissue or the fibrous connective tissue replaces the muscle fibers, resulting in the generalized atrophy of the muscles 11. The atrophy of masticatory musculature results in reduction in the ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Tongue:
In general, it is a common observation that there is a little change in the vascularity of the tongue with increasing age 12. The observation regarding the atrophy of the papillae, altered taste sensation and increased tendency for fissure formation on the tongue with increasing age are controversial 13-15. The earlier studies reported a decrease in the number of taste buds with increasing age 16, however, studies done later on, discarded this finding and observed no significant change in the number of taste buds with increasing age 17.
Decreased taste sensitivity has been reported with increasing age in many studies, however, the reason for this has not been well explained. Research has indicated that there is a decrease in taste sensitivity after the age of 55 years 18. One study has reported that more taste buds are required to perceive the taste sensation in elderly individuals as compared to children 19. Another explanation for decreased taste sensitivity in elderly people is decrease in the salivary flow with increasing age. The taste buds react only to dissolved compounds. Sweet and salty taste sensation perceived by the tongue have been reported to deteriorate prior to the sour and bitter sensation 20, 21.
Salivary glands:
In the past, it was a general opinion that salivary flow reduces with increasing age. However, recent studies have reported that a decreased salivary flow with increasing age in primarily because of pathologic conditions or pharmacologic effects of medications rather than aging 9, 22-24. Still, more research is required on this topic to establish a clear correlation between aging and salivary flow.
Pathological changes in the oral and peri-oral tissue in elderly individuals
Pathological changes in the oral and perioral hard tissues
Alveolar bone:
The decrease in the mineral content of the alveolar bone with increasing age results in increased porosity and atrophy of the bone. The most common pathological reason for the loss of alveolar bone is periodontitis. Elderly individuals commonly have chronic periodontitis which is a slow progressing disease-causing alveolar bone loss over many years. This bone loss can be minimized with appropriate treatment of the patient and supportive periodontal therapy.
Another reason for decreased bone mass is osteoporosis, especially in post-menopausal females. One of the initial signs of osteoporosis is alveolar bone loss which is followed by bone loss in the vertebrae and long bones 25. This bone loss may result in ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Teeth:
Dental caries:
In elderly individuals, caries is most commonly seen around the restoration margins, root surfaces, and cervical caries at the gingival margins 28, 29. Recession on the tooth-root surfaces with increasing age is the main cause of root caries. The recurrent caries is most commonly found in the inter-proximal areas 30. Other factors that contribute to the root and cervical caries include poor oral hygiene, decreased salivary flow and diet. Xerostomia has been significantly associated with increase rate of root surface caries. In elderly individuals the most common causes of xerostomia include medications, head and neck radiation for malignancies and Sjögren’s syndrome 31.
Various strategies have been used to prevent the development of root surface caries which include improvement of oral hygiene, chemical plaque control measures and topical fluoride application. Daily topical application of ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Abrasion:
Faulty brushing technique results in gingival recession and cervical abrasion of teeth. An important cause of abrasion is overzealous brushing with hard tooth brush. The abrasion on the right or the left side of the dentition depends on whether the individual is right or left-handed. For right-handed individuals the abrasion occurs on the left side of the dentition due to excessive pressure during brushing and vice versa for left-handed individuals. Tooth abrasion can be prevented by modifying the brushing technique and by using soft bristle tooth brushes. Other causes of tooth abrasion include faulty use of dental floss and toothpicks. Patient should be told to use the interdental cleansing aids properly to prevent tooth abrasion.
Erosion:
Tooth erosion is the wear of tooth structure by chemical dissolution. If the concentration of acid in mouth increases to an extent where it cannot be neutralized by saliva, tooth structure is lost due to dissolution. The most common causes of erosion include ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
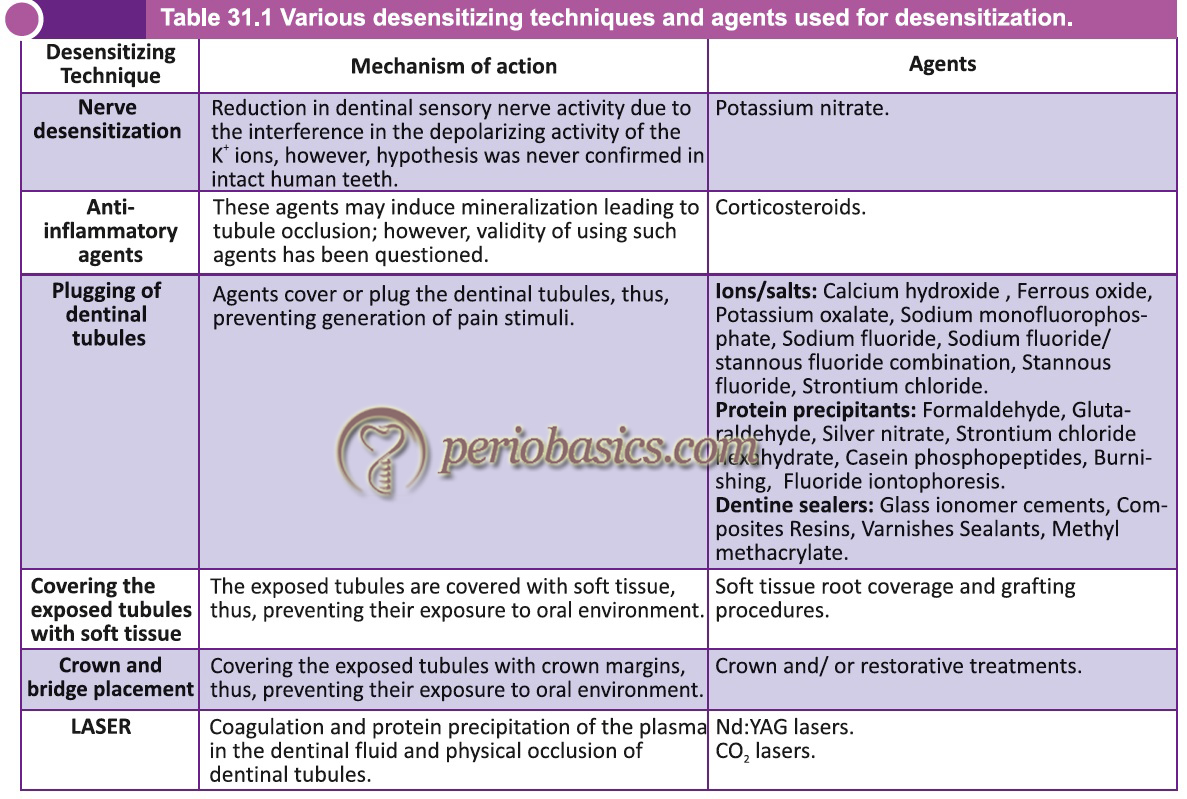
Dentinal hypersensitivity:
One common dental problem faced by elderly people is the dentinal hypersensitivity. The cause for the dentinal hypersensitivity is primarily the exposure of the dentinal tubules due to abrasion, erosion, acute or chronic trauma, or various restorative treatment procedures. The teeth may become sensitive to thermal, chemical, tactile or osmotic stimuli. Severe dentinal hypersensitivity may prevent an individual to properly maintain oral hygiene, thus, its treatment should be done on a priority basis. Various methods can be used to treat dentinal hypersensitivity which have been summarized in the following table,
Tooth loss:
In elderly patients missing tooth/teeth is a common finding. The loss of the tooth may be associated with periodontal or dental problems in the past. The rate of tooth loss increases with age. Due to loos of tooth/teeth, these patients often complain of the difficulties during chewing. A careful history should be recorded to elicit the cause of tooth loss. This is because in patients who give a history of tooth loss in past due to periodontal disease are at a greater risk of development of periodontal disease in future. However, it should be noted that at present, the rate of edentulism has reduced as compared to past due to improvement in dental health services and patient awareness 45, 46.
Temporomandibular Joint (TMJ):
A detailed description of the physiology of TMJ has been given in “Temporomandibular joint and occlusal considerations in periodontics”. The TMJ problems are more commonly encountered in elderly as compared to younger individuals 47. The patients may complain of tenderness or pain of the masticatory and facial muscles, dull, aching facial pain, severe pain in the joint area, popping, clicking, or cracking noises near the ear while opening and closing the mouth, dizziness, headaches, impaired hearing or earache 47, 48. According to Peck et al. (2014) 49, the disorders associated with TMJ are given in the following table,
I. TEMPOROMANDIBULAR JOINT DISORDERS
1. Joint pain
A. Arthralgia
B. Arthritis
2. Joint disorders
A. Disc disorders
1. Disc displacement with reduction
2. Disc displacement with reduction with intermittent
locking
3. Disc displacement without reduction with limited opening
4. Disc displacement without reduction without limited
opening
B. Hypomobility disorders other than disc disorders
1. Adhesion/adherence
2. Ankylosis
a. Fibrous
b. Osseous
C. Hypermobility disorders
1. Dislocations
a. Subluxation
b. Luxation
3. Joint diseases
A. Degenerative joint disease
1. Osteoarthrosis
2. Osteoarthritis
B. Systemic arthritides
C. Condylysis/idiopathic condylar resorption
D. Osteochondritis dissecans
E. Osteonecrosis
F. Neoplasm
G. Synovial chondromatosis
4. Fractures
5. Congenital/developmental disorders
A. Aplasia
B. Hypoplasia
C. Hyperplasia
II. MASTICATORY MUSCLE DISORDERS
1. Muscle pain
A. Myalgia
a. Local myalgia
b. Myofascial pain
c. Myofascial pain with referral
B. Tendonitis
C. Myositis
D. Spasm
2. Contracture
3. Hypertrophy
4. Neoplasm
5. Movement disorders
A. Orofacial dyskinesia
B. Oromandibular dystonia
6. Masticatory muscle pain attributed to systemic/central
pain disorders
A. Fibromyalgia/ widespread pain
III. Headache
Headache attributed to TMJ
IV. Associated structures
Coronoid hypoplasia
Pathological changes in the oral and peri-oral soft tissue
Mucous Membranes/Epithelium:
The oral cavity is an open cavity. In the oral cavity, both keratinized and non-keratinized epithelium are present. The moist environment in the oral cavity provides an ideal environment for the proliferation of microorganisms of various strains and species. Furthermore, oral cavity is subjected to a variety of thermal, chemical and mechanical insults throughout the lifetime of an individual. But, because of good healing capability, the oral mucosa is healed within a short period of time depending on the type of injury. In elderly individuals, a variety of changes are observed in the oral and peri-oral tissues discussed as follows.
Aphthous Ulcer:
Aphthous ulcer is also referred to as aphthous stomatitis, ulcerative stomatitis or canker sore. These are inflammatory lesions of the oral mucous lining which may involve the gingiva, tongue, lips, buccal mucosa, roof or floor of the mouth and oropharynx. These are usually painful and associated with redness, swelling, and occasional bleeding from the affected area. The ulcers are usually covered with a pseudomembrane. These are usually painful and interfere with eating and swallowing. Etiology of oral apthous ulcers is largely unknown. Various factors such as stress, trauma, nutritional deficiencies, food components, and allergies have been shown to be contributory to the disease 50- 51. The ulcers usually ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Candidiasis:
The most common opportunistic fungal infection, regardless of patient’s age, is candidiasis. It is caused by the overgrowth of a species of fungus Candida. The most common species of candida implicated for oral candidiasis is Candida albicans. There are various clinical forms of oral candidiasis. These include acute pseudomembranous candidiasis (thrush), acute atrophic candidiasis (antibiotic sore mouth), or chronic atrophic candidiasis (denture sore mouth), angular cheilitis and rarely chronic hyperplastic candidiasis and chronic mucocutaneous candidiasis. In immunocompromised elderly patients candidemia and invasive candidiasis may also occur due to systemic invasion of the Candida species.
Pseudomembranous candidiasis or ‘thrush’, involves opportunistic fungal invasion of the most superficial layers of the squamous mucosa resulting clinical in the formation of creamy white or yellowish plaques that are fairly adherent to oral mucosa. On removal of the plaque by scraping, erythematous base or a bleeding surface usually appears. It is most commonly found on the palate, buccal, and labial mucosa, and on the lateral borders and dorsum of the tongue.
Atrophic candidiasis (acute or chronic) clinically appears as fiery red flat lesions on the palate, patchy areas of loss of filiform papillae on the dorsum of the tongue, or spotty red areas on the buccal mucosa. The denture associated candidiasis is present under the removable prosthesis. The lesion usually appears smooth, ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Hyperplastic form of candidiasis is rare and involves invasion of deeper tissues followed by a hyperplastic response. This type of candidiasis is also referred to as candidal leukoplakia. This form may also clinically present as mixed red and white areas which may have dysplastic potential.
Chronic mucocutaneous candidiasis is usually associated with long-standing and persistent candida infection of the mucocutaneous tissues. This type of candidiasis has been linked to a spectrum of immunologic, endocrinologic, and autoimmune disorders. The unifying feature of these heterogeneous disorders is impaired cell-mediated immunity against Candida species.
Leukoplakia:
Leukoplakia is defined as a predominantly white lesion of the oral mucosa that cannot be characterized as any other definable lesion. The lesion may vary from a small circumscribed area to an extensive lesion involving a large area of mucosa and can occur in any part of oral mucosa. The incidences of leukoplakia are highest in the fifth to seventh decade of age 52. The etiology of leukoplakia is unknown. However, a variety of smokeless tobacco habits have been associated with the development of this condition. The lesions have been shown to have a tendency for malignant transformation.
Classically, leukoplakia has been classified as homogeneous and non-homogeneous. The homogeneous type is characterized by a thin, flat and homogeneous whitish appearance whereas non-homogeneous type is further subdivided into speckled, nodular and verrucous leukoplakia 53. The speckled type is a white and red lesion, with a predominantly white surface. The verrucous leukoplakia has an elevated, proliferative or corrugated surface appearance. The nodular type has small polypoid outgrowths, rounded predominantly white excrescences.
Various non-surgical treatments options for oral leukoplakia include ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Oral mucositis and stomatitis:
Although mucositis and stomatitis terms can be used interchangeably, however, stomatitis has usually been connected with non-cancer- related oral conditions whereas mucositis term is usually used to describe the lesions caused by anticancer agents. The condition is characterized by painful inflammation, erythema, swelling, and ulcerations of the oral mucosa in the oral cavity, oropharynx, and hypopharynx. The pathogenesis of oral mucositis is not fully understood, yet it is thought to involve direct and indirect mechanisms. The direct mechanisms involve injury by radiation and chemotherapy which interferes with the average 5- to 14-day turnover time of the oral epithelium, inducing their apoptosis 54. Indirect mechanisms involve the release of inflammatory mediators resulting in the injury to the cells, resulting in mucositis.
The treatment for the condition is symptomatic. Local anesthetic and antacid preparations are used singly or in combination to relieve the pain and discomfort associated with stomatitis. The use of mouth rinses is discouraged because they have an irritating and desiccating effect on oral mucosa. Radiation-induced mucositis is associated with pain, burning sensation, and discomfort during eating and swallowing. After the therapy, mucositis usually resolves within several weeks, however in the meantime, the use of liquid topical anesthetics in the mouth before mealtimes is recommended to reduce discomfort during eating.
Denture related pathologies:
Dentures rest on the oral mucosa and their cleanliness is essential to ensure the health of oral mucosa. Accumulation of plaque, food debris, and calculi on and around the denture surfaces causes irritation, inflammation and infection in the surrounding tissue and promotes halitosis. It has been observed that in long term; partial dentures contribute to increased plaque formation around abutment teeth thus, promoting inflammation 55. Furthermore, the use of removable prosthetic appliances promotes tooth mobility and bone loss so their cleanliness becomes even more important. The patients using complete or removable partial dentures should be advised to keep their appliances clean and get their appliances replaced with new one, when required.
Denture stomatitis is the condition in which there is generalized inflammation associated with denture wearing. The exact etiology of this condition is unknown, however, various suggested etiologies include contact hypersensitivity to dental materials, bacterial and candidal infections, tissue reaction to ill-fitting or unclean dentures, residual denture cleanser, medication use, and systemic diseases 56, 57. Denture stomatitis is more severe in patients who do not remove the denture at night or do not maintain denture cleanliness. The disease is resolved with a thorough cleaning of the denture or replacement of an ill-fitting denture.
Ill-fitting dentures may also result in ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Pathologies associated with tongue:
Glossitis:
It is the inflammation of tongue that results due to considerable atrophy of the filiform papillae. Glossitis may also be caused by a variety of diseases including nutritional deficiency, anemia, drug reactions, celiac disease, systemic infection, and physical or chemical irritations. Other less common etiologies of the disease are amyloidosis , protein-calorie malnutrition, and xerostomia triggered by some medications and Sjögren syndrome. Treatment includes replacement of the missing nutrient or treatment of the underlying condition 58-60.
Glossodynia and Glossopyrosis:
Glossodynia or pain in the tongue, and glossopyrosis or burning tongue are commonly seen among elderly individuals. The patient complains of difficulty in eating and swallowing. One important feature of “burning mouth syndrome” is atrophy of the tongue papillae. The exact etiology of these conditions is not clear but pernicious anemia, nutritional disturbances, emotional disturbance, hormonal imbalance, allergies and some psychosomatic syndromes have been found to be precipitating factors. Treatment for these conditions is identification of the underlying cause and its elimination. However, in most of the cases the underlying cause cannot be identified and treatment is only symptomatic.
Hairy tongue:
Hairy tongue is more common in elderly individuals as compared to younger individuals. It is a temporary and harmless condition which is characterized by elongated, thick, densely matted, and stained filaments on the dorsum of the tongue that resemble hair. The exact pathogenesis is unclear, however, a number of factors have been identified which may act as precipitating factors for hairy tongue including poor oral hygiene, hyposalivation, smoking, intake of alcohol, use of topical or systemic antibiotics as well as psychotropic agents, dehydration, trigeminal neuralgia, and ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Pathologies related to salivary glands:
Sialolithiasis:
Sialoliths or salivary stones are calcified structures or concretions located in any of the major or minor salivary glands or their excretory ducts. These obstruct the salivary secretion, resulting in symptoms such as pain and swelling in the submandibular or parotid region during mealtime. Pain and swelling are more common when the stone is located in the duct than when the stone is located in the gland itself 61. The etiology of these calculi is little known and their exact mechanism of formation is unknown, however various hypothesis have been put forward for their formation. These include the agglomeration of sialomicroliths, anatomical variations of the salivary ducts and an altered biochemical composition of saliva. It has been proposed that a decreased flow of saliva causes precipitation of calcium in the salivary ducts, resulting in calculi formation 62. Structurally, sialoliths are composed of amorphous, mineralized core or nucleus, with concentric laminated layers or shells of organic and inorganic substances 63-66. The non-invasive treatment for sialoliths includes gland massage, in combination with use of sialogogues and irrigation. It is done when the sialolith is small and located near the duct. Invasive management of sialolithiasis may consist of extracorporeal shock-wave lithotripsy, sialoendoscopy or surgical removal.
Xerostomia:
Xerostomia is the subjective sensation of dry mouth which is commonly observed in elderly individuals. It is frequently but not always associated with salivary hypofunction. The patients with xerostomia usually complains of dryness in mouth, increased plaque accumulation, rampant caries, sticking of food or lips to the teeth, unsatisfactory chewing of food, difficulty in speaking, nocturnal discomfort, glossodynia or glossopyrosis, cracking of lips, altered taste sensation and injuries of oral mucosa.
There are various etiological factors that may be associated with the development of xerostomia. Medical conditions which result due to autoimmune reactions, degenerative and granulomatous disorders and certain infections have been found to be associated with xerostomia. Another common cause of xerostomia is medications which interfere with the transmission of signals at the parasympathetic neuro effector junctions or interfere with actions at the adrenergic neuro effector junctions or cause the depression of the connections of the autonomic nervous system. This effect of these medications is reversible and salivary flow becomes normal as soon as the drug is discontinued.
| Causes of xerostomia | |
|---|---|
| Medical conditions associated with xerostomia | Autoimmune and inflammatory conditions (such as Sjögren syndrome or primary biliary cirrhosis), Graft-versus-host disease, Immunoglobulin G4-related sclerosing disease, Degenerative disease (amyloidosis), Granulomatous disease (sarcoidosis) Infections: human immunodeficiency virus/AIDS, hepatitis C, Salivary gland aplasia or agenesis, Lymphoma |
| Medications frequently associated with xerostomia | Drugs that directly damage salivary glands: Cytotoxic drugs, Drugs with anticholinergic activity: Anticholinergic agents: atropine, atropinics and hyoscine, Antireflux agents: proton-pump inhibitors (e.g., omeprazole), Central-acting psychoactive agents: Antidepressants, including tricyclic compounds, Phenothiazines, Benzodiazepines, Antihistamines, Bupropion, Opioids, Drugs acting on sympathetic system: Drugs with sympathomimetic activity (e.g., ephedrine), Antihypertensives: α-1 antagonists (e.g., terazosin and prazosin); α-2 agonists (e.g., clonidine); may reduce salivary flow, β blockers (e.g., atenolol, propanolol), which also alter salivary protein levels Drugs that deplete fluid: Diuretics |
| Other causes | Local radiation, Chemotherapy |
Another common cause of xerostomia is radiation therapy which is given for the treatment of neoplasms of head and neck region. If given as a single dose, a radiation dose as low as 20 Gy can cause permanent cessation of salivary flow. The most radiosensitive salivary gland is parotid gland follo-wed by submandibular, sublingual and minor salivary gland.
There are various problems associated with decreased salivary flow. Saliva performs various functions in oral cavity including lubrication, cleansing action, buffering action, remineralization and antibacterial action. An individual with xerostomia is at high risk of developing traumatic injury to oral mucosa, caries, periodontal diseases, glossitis, abrasion and erosion of tooth surfaces, altered taste sensation, infections associated with pharynx and salivary glands and difficulties involved with chewing and swallowing 67. In patients wearing complete dentures or removable partial dentures, xerostomia magnifies the prosthesis related problems as saliva is required to make a seal between the denture and underlying tissues. Further, due to decreased salivary flow there are more chances of tissue injury caused by denture abrasion.
The management of xerostomia is done at ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Intraoral topical agents:
These agents include chewing gums, saliva stimulants, and substitutes. They provide symptomatic relief by improving the hydration of the oral cavity. Recently, a spray containing 1% malic acid has been introduced; however, it may result in the loss of the tooth structure. Oxygenated glycerol tri-ester oral sprays have been found to be useful for the treatment of xerostomia cases. Saliva substitutes, such as carboxymethyl-cellulose or hydroxyethylcellulose with flavoring agents, and preservatives are useful in providing symptomatic improve-ment in xerostomia patients.
Systemic sialogogues:
Pilocarpine and cevimeline are the two systemic sialogogues used for treatment of dry mouth. The prerequisite for the use of these medications is the presence of functional glandular tissue. The mechanism of action of these medications is not similar. Pilocarpine is a parasympathomimetic medication with muscarinic action 68, 69 whereas cevimeline is a salivary gland stimulant with a stronger affinity for M3 muscarinic receptors 70-72. The dosage of Pilocarpine is 5 mg three times a day for at least 3 months and for cevimeline it is 30 mg three times a day for at least 3 months 73. The use of these drugs is contraindicated in patients taking β-adrenergic blocker and in patients with uncontrolled asthma or chronic pulmonary disease. The side effects associated with the use of these medications include bronchoconstriction, hypotension, bradycardia, excessive sweating, cutaneous vasodilatation, increased urinary frequency, and vision problems.
Oral cancers:
The neoplasms of oral cavity can significantly affect the chewing capability and usually result in significant discomfort to the patient. In general, the prevelance of oral cancer has been found to be significantly more in males as compared to females. This difference is primarily due to more use of tobacco products by males as compared to females. The treatments of neoplasms include chemotherapy, radiotherapy and surgical treatment.
In many patients with oral cancer, radiotherapy is done. It commonly results in radiation-induced soreness, xerostomia, and taste loss. With chemotherapy, there is a loss of ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Periodontal problems in elderly individuals
Most of the elderly population has been observed to suffer from one or another type of dental or periodontal problem. Periodontal problems are disorders that affect the gingiva, supporting connective tissue, and alveolar bone. In general, the prevalence of periodontal problems increases with age 74-77 and is higher in elderly individuals than in young individuals 78. In a review, Locker et al. (1998) 79 concluded that approximately 70% of older adults demonstrate evidence of advanced periodontitis, but the number of affected sites/teeth is small. When observed longitudinally, the periodontal disease progression is observed at newly affected sites as opposed to continued loss at previously affected sites. Cigarette smoking and the presence of specific periodontal pathogens were found to be the most important risk factors for periodontal disease progression in elderly patients.
In a study on community-dwelling individuals in Sweden (with minimum age of 80 years), Holm-Pedersen et al. (2006) 80 reported that ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Approach to treatment
The treatment protocol for periodontal problems in elderly patients are addressed in five steps,
1. Examination of the patient and emergency treatment.
2. Cause-related therapy.
3. Re-evaluation of the patient.
4. Definitive treatment.
5. Maintenance phase.
Examination of the patient and emergency treatment
Recording of the case history is an essential step for accurate treatment planning. The patient’s chief complaint or active problems are recorded followed by a thorough clinical examination. The medical history of the patient should be recorded to find out any underlying medical condition such as diabetes mellitus etc. Elderly patients are commonly on medication for one or the other kind of medical problem. The medical condition should be identified and the medications should be noted down. The socioeconomic status of the patient should be identified. Psychological status of the patient should be examined to identify any mental stress.
Dental history of the patient should be recorded to find out the previous dental treatments, the patient has undergone. In elderly patients, missing teeth is a common finding. The reason of tooth loss should be identified. As already stated, a previous history of periodontitis is considered as a risk factor for future periodontal breakdown. The present status of the dentition should be recorded with occlusion related findings.
The periodontal examination should be done by checking the probing depth, clinical attachment loss, presence of bleeding on probing, tooth mobility, pathological ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Cause-related therapy:
Cause-related therapy involves elimination of the local factors including plaque and calculus. Scaling and root planing is done to remove all the local factors present. The home oral hygiene maintenance measures used by the patient are identified and patient is demonstrated a correct brushing technique, if required. In elderly patient, reduced dexterity and/or sensory impairment adversely affect their capability to maintain adequate oral hygiene. Additional oral hygiene aids or modification in currently used aids is required in these patients to ensure good oral hygiene. It should be noted here that recommending a powered toothbrush to these patients is indicated, but care should be taken to ensure that the toothbrush is not too bulky and heavy as it would limit or preclude their effective use. If the mechanical plaque control measures are ineffective in the maintenance of adequate oral hygiene, chemical plaque control measures such as chlorhexidine gluconate can also be advised to the patients.
Re-evaluation of the patient:
The patient is re-evaluated and improvement in periodontal status of the patient is noted. It is important to note here that if the patient is not able to maintain adequate oral hygiene, the reason for the same should be identified. The patient should be re-instructed regarding the home care procedures and again put on recall to evaluate any improvement. Once it is made sure that patient is able to maintain adequate oral hygiene, the future course of the treatment is planned. If there are remaining periodontal pockets, various non-surgical and surgical options should be explored and option best suitable for a particular patient should be explained to the patient.
In general, there may be three outcomes of the initial periodontal treatment. These are,
- Periodontal stability is achieved and there is no sign of active periodontal disease. In such case, the patient is put on maintenance therapy and is recalled at a regular interval to re-evaluate the periodontal status.
- Patient has moderate to deep pockets (≥ 4 mm) which cannot be maintained by home care procedures; however, there is no bleeding on probing and no sign of active periodontal destruction. In such cases, it is possible that the healing process is going on in the pocket and injudicious premature instrumentation of the root surface may result in interference with the healing process. Thus, only promotion of oral hygiene and scaling and root planing is required. However, the patient is recalled in shorter intervals (1-2 months) for maintenance therapy. It should be remembered that if any site demonstrates signs of active periodontal destruction, it should be aggressively addressed.
- Periodontal stability cannot be achieved and signs of active disease are present. If it is observed that further treatment is unlikely to improve the periodontal support of the involved tooth/teeth and their medium to long term stability is questionable, then treatment of choice is extraction and replacement of tooth/teeth with removable or fixed prosthetic appliance. On the other hand, if it is observed that periodontal treatment can achieve periodontal stability and involved tooth/teeth is expected to be functional for long term, non-surgical or surgical periodontal therapy can be planned for the patient, that is safe for the patient and patient wishes to have. However, it should be remembered that if surgical therapy is planned, flap procedures that result in minimum post-operative gingival recession should be chosen to avoid tooth root exposure that may facilitate development of root surface caries.
Definitive treatment:
In this phase of treatment, the additional non-surgical or surgical therapy planned in the re-evaluation phase, are executed. It must be remembered that the surgical therapy should be ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Maintenance phase:
Periodontal diseases are the result of host-microbial interaction. The microbial film constantly forms on the surface of teeth, so it may result in recurrence of the disease. This means that maintenance therapy is essential to prevent the progression of periodontal disease. According to Kerry (1995) 81, there are three objectives of supportive periodontal therapy,
- To prevent the progression and recurrence of periodontal disease in patients who have been previously treated for gingivitis and periodontitis;
- To reduce the incidence of tooth loss by monitoring the patient’s dentition;
- To increase the probability of recognizing and treating other diseases or conditions found within the oral cavity.
Various longitudinal studies on surgical and non-surgical periodontal therapy have demonstrated that patients who strictly follow the periodontal maintenance therapy have less average tooth loss per year as compared to those who do not. Details of these studies have been given in “Periodontal maintenance”.
How effective is periodontal therapy in geriatric patients?
Various studies have demonstrated that age is not an important criterion for the determination of success rate of periodontal treatment 82-84. The results of periodontal therapy are primarily dependent on the post-treatment self care by the patient and strict adherence to the maintenance protocol. It should be noted here that if an elderly patient has majority of ……….. Contents available in the book ……….. Contents available in the book……….. Contents available in the book……….. Contents available in the book……
Problems in providing oral health care to geriatric patients
There are many challenges in providing oral health care to geriatric patients. One of the most important factors are the overall awareness and social background of the patient. The awareness of the patient regarding oral health care depends on the availability of oral health care facilities in the area where the patient has spent most of his/her lifetime. A patient regularly visiting a dentist or health care provider is much more aware of oral health problems as compared to a patient who had little access to the oral health facilities. Along with this, there are many other factors associated with elderly patients, which make the delivery of oral health care difficult in these patients. These include,
Health-related factors:
- General ill health.
- Mobility, functional limitation.
Social and demographic factors:
- Ethnicity
- Culture
- Education
- Income
Service-related factors:
- Accessibility to health services.
- Satisfaction with service.
- Behavior of the health care provider.
Patient-related factors:
- Personal beliefs.
- Fear and anxiety.
- Financial strain.
- Feeling of no need for the treatment.
To overcome these problems, a personalized approach should be used to treat every patient. The problems associated with a particular patient should be analyzed carefully and the patient should be motivated to maintain a good oral hygiene. Appropriate treatment should be provided to the patient and maintenance recalls should be planned carefully.
Conclusion
The population of elderly individuals is increasing throughout the world due to improvement in the medical facilities. Thus, management of periodontal problems in elderly patients becomes increasingly important and relevant. However, it should be remembered that the therapeutic choices should be made in elderly patients on individual basis taking into consideration their age, dental and medical status, goals to be achieved and long term maintenance. In the above discussion, a logical approach has been discussed to address the periodontal problems faced by geriatric patients. If utilized appropriately, these patients can be efficiently treated and maintained for long term with this approach.
References
References are available in the hard-copy of the website,
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users: