Introduction to periodontal maintenance
Periodontal diseases are multifactorial diseases where host-microbial interactions lead to the destruction of periodontal soft and hard tissues. Various forms of periodontitis can be efficiently treated with non-surgical and surgical therapy, but periodic periodontal maintenance is important for the maintenance of periodontal health after active periodontal treatment. Periodontal maintenance is defined as the procedures that are performed at selected intervals after active periodontal treatment to assist the periodontal patient in maintaining oral health. The term periodontal maintenance can be used interchangeably with the term supportive periodontal therapy. However, in a position paper by the American Academy of Periodontology, term periodontal maintenance was preferred over supportive periodontal therapy 1.
Periodontal maintenance is an integral part of periodontal treatment and is performed at regular intervals on the patient by the dentist, although some components of the treatment can be performed by a dental hygienist under the supervision of the dentist. Periodontal maintenance involves a periodic review of the medical and dental status of the ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Rationale for periodontal maintenance
There is a large body of evidence in favor of periodontal maintenance therapy. To understand the rationale for perio-dontal maintenance therapy, we must find out the answers to some questions. Let us start by discussing, what happens if periodontal disease is not treated?
Waerhaug (1952) 2 demonstrated that the retained supra-gingival plaque develops an “advancing plaque front” which progresses to develop subgingival plaque. Later on, it was highlighted that there is a cause and effect relationship between the accumulation of subgingival plaque and development of gingivitis and periodontitis 3, 4. These findings led to many longitudinal ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
A landmark study highlighting the relationship between the accumulation of local factors in the development of inflammatory periodontal diseases was done by Loe et al. (1986) 5 on Srilankan tea workers. It was a 15-year observational study on 480 male tea plantation workers aged 14-31 years, who never had any access to any kind of prophylactic or interventional dental care. These patients were re-evaluated after every three years and after 15 years 161 patients were available who had participated in the study. The authors observed that there was a large accumulation of plaque and calculus in the patients and reason for tooth loss was primarily the periodontal bone loss rather than caries. On the basis of rate of progression of disease, three patient groups were recognized,
- Subjects with rapid progression of periodontal diseases (8%).
- Subjects with moderate progression of the disease (81%).
- Subjects with no disease progression (11%).
The annual rate of attachment loss in subjects with rapid, moderate and no disease progression was 0.1-1.0 mm, 0.05-0.5 mm and 0.05-0.09 mm respectively.
In another study Backer et al. (1979) 7 examined 30 patients diagnosed with moderate to advanced periodontal disease. During the study duration, subjects did not receive any periodontal treatment. Tooth loss and probing depths were recorded during the course of the study. The authors reported an inverse relationship between probing depth increase and patient age. In the most severe case, the patient lost 25 teeth during the observation period. The mean tooth loss calculated was ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Now, let us discuss the difference between periodontal status and tooth loss in patients who are not treated for periodontal disease and those who are put on a regular periodontal maintenance therapy.
In a study, Buckley and Crowley (1984) 6 studied 1,016 textile workers for a period of 10 years. The results of the study showed that subjects who did not receive any periodontal treatment during the study period had an average tooth loss of 2.5 teeth per subject which was 2-12 times higher than the subjects who received periodontal treatment. The periodontal diseases also displayed ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
In another 7 year longitudinal study on Indonesian population, Timmerman et al. (2001) 8 investigated the role of clinical and microbiological putative factors in periodontal disease progression. The subjects enrolled in the study had no access to dental care. Plaque index, bleeding on probing (BOP), pocket depths and attachment loss were recorded for each patient on selected teeth. Pooled plaque samples from the deepest pockets in each quadrant, dorsum of the tongue, buccal gingiva, and saliva were evaluated by phase contrast microscopy and immunofluorescence. The results of the study showed that all the clinical parameters except probing depth increased during the course of study. Microbiological investigations revealed an increased prevalence of periodontal pathogens, including Aggregatibacter actinotnycetemcomitans (40%), Porphyromonas gingivalis (67%), Prevotella intermedia (66%), Fusobacterium nucleatum (79%), and Bacteroides forsythus (16%). The authors concluded that ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Now, let us try to find out that what happens to the periodontal status of patients who are treated and not maintained?
Nyman et al. (1977) 9 in a study on 25 patients with advanced periodontal disease observed the progression of periodontal disease where after periodontal treatment, no periodontal maintenance was provided. Patients were treated by one of the five procedures to eliminate probing depth. Patients were instructed regarding maintenance of oral hygiene once and were not recalled for maintenance. The evaluation of the patients was done at 2, 6, 12, and 24 months. The results of the study showed that ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
In another study, Becker et al. (1984) 10 observed the periodontal status of 44 patients (1,117 teeth) treated for periodontal disease and who did not participate in the maintenance phase of treatment. The patients were given oral hygiene instructions, initial scaling and root planing was done and pocket reduction therapy was done in two or more quadrants. The average time between examinations was 5.25 years. The authors reported an average tooth loss of 0.22 per year in these patients as compared to 0.11 in patients who were treated and received maintenance therapy. Annual average tooth loss for diagnosed and untreated patients was 0.36. Patients without maintenance therapy demonstrated progressive furcation involvements, no reduction in probing depth and worsening of bone scores. In was concluded that the surgical therapy is of little value in the absence of periodontal maintenance therapy.
Kocher et al. (2000) 11 in a study demonstrated that patients who did not participate in the periodontal maintenance demonstrated progressive interdental bone loss and increased rate of tooth loss as compared to patients who participated in maintenance therapy. The authors concluded that periodic periodontal maintenance treatment arrested the interdental bone loss and reduced the rate of tooth loss in most of the cases. Further, it was also concluded that ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
The importance of recall visits for preventing progression of periodontal destruction in patients who have undergone active periodontal treatment was further emphasized by many other researches 12-15.
Lastly, the final question is what is the periodontal status of patients who are treated for periodontal disease and are on regular periodontal maintenance?
Hirschfeld and Wasserman (1978) 16 examined the well-kept records of 600 patients who were maintained by periodontal maintenance therapy for an average of 22 years. The active treatment of the patients included scaling/root planing, hemisection and flap surgery. Following the active periodontal treatment, the patients were put on periodontal maintenance recall visits every 4-6 months. During recall visits probing depth, mobility and furcation involvement was recorded. The results of the investigation revealed that well-maintained patients (83% of all patients) had 0-3 tooth loss, moderately maintained ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
In a similar study, which examined patient’s periodontal status for an average of 19 years, McFall observed that during maintenance phase the average tooth loss was 0.13 per year. It was noted that during appropriate periodontal maintenance, only 9.8% teeth were lost due to periodontal disease. Further, it was observed that more than half of the teeth with furcation involvement were lost during this period. The well-maintained patients lost 27% of the furcation involved teeth; while moderately ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
These observations have been supported by many other studies which have examined the patients who are on periodic periodontal maintenance and those who are not 12, 17-19.
Effect of periodontal maintenance on gingivitis
Many studies 12, 17, 20-22 have evaluated the effect of periodic periodontal maintenance on gingival inflammation. Lövdal et al. (1961) 23 did a 5-year study on 1428 adults. During the duration of the study, the subjects were recalled for re-evaluation 2-4 times per year. During these appointments, subjects were reinforced regarding the maintenance of oral hygiene and supra and subgingival scaling was done. The authors reported 60% improvement in gingival condition and 50% reduction in tooth loss. In another 3 year study, Suomi et al. (1971) 24 investigated the effect of regular periodontal maintenance on gingival inflammation and attachment loss. The experimental group was put on three-month periodontal ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ………
Effect of periodontal maintenance on periodontitis
Various long term studies were done in the late 60’s continuing into the 70’s and 80’s which compared the long-term outcome of periodontal surgical and non-surgical procedures. These studies were done by various group of researchers and are recognized by their geographic location, such as, Michigan study I, II, and III 19, 25-30, Swedish study I, II, III, IV, and V 31-38, Minnesota study 39-41, Denmark study 42, 43, Loma Linda study 44-59, Arizona study 60-62, Nebraska study 63-65, and others. It was known at that time that both non-surgical and surgical periodontal therapy results in improvement in periodontal condition, but their long-term outcome was not documented. The primary aim of these studies was to compare the effects of two or more therapies on various clinical parameters including plaque accumulation, bleeding upon probing, probing depth, probing ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
These studies included patients who were regularly recalled for periodontal maintenance and who were maintaining a good oral hygiene. Although these patients performed plaque removal with various degrees of efficacy, the professional periodontal maintenance resulted in highly favorable results in terms of post-operative maintenance of attachment levels in most of the patients 19, 66. The authors in the Swedish study (Gothenburg) concluded that the patients who were treated with surgical periodontal therapy, but not incorporated into a supervised periodontal maintenance therapy regime, exhibited ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Objectives of periodontal maintenance therapy
The primary objectives of periodontal maintenance therapy are,
- Assessment of oral hygiene maintenance by the patient and elimination of local factors and plaque.
- Early recognition and prevention of the disease recurrence.
- Preventing the progression of the disease if present.
- Prevention of recession.
- Reducing the incidence of tooth loss by monitoring the dentition and providing any prosthetic replacements for the missing natural teeth.
- Maintenance of healthy and functional oral environment by monitoring any changes in the dentition and oral cavity.
- Increasing the probability of locating and treating, in a timely manner, other diseases or conditions found within the oral cavity.
- Re-evaluation and reinforcement of effective plaque control by the patient.
Continuous multi-level risk assessment
Once the active periodontal treatment is completed, the parameters determining periodontal maintenance or supportive periodontal therapy are entirely different from parameters with which the patient initially reported with active disease. The periodontal disease is treated with non-surgical and /or surgical periodontal therapy and the patient is reassessed for periodontal status and other factors influencing the disease progression. The clinical attachment levels achieved after adequate periodontal treatment have to be maintained for as long as possible, so they are recorded. Since inflammation of the gingiva is the first sign of periodontal disease progression, gingival status is recorded. The periodontal environment is very dynamic and there are various factors which determine periodontal health. Most important of these factors are the host and microbial interactions. Following periodontal treatment, an equilibrium is achieved between both of these factors, which favor the ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
It must be emphasized here that patients who have already been treated for periodontal disease are at more risk of recurrence of the disease as compared to the general population. These patients need to participate in a well-organized maintenance program, in the absence of which the recurrence of disease has been shown to be more likely 13-15. The individual risk assessment determines the frequency of calling a patient for professional support so that the initiation of periodontal disease may be stopped.
In multi-level risk assessment, the risk assessment is done at three levels: at subject level, at tooth level and at site level. Let us now discuss them in detail,
Subject risk assessment
A computer-based risk assessment tool was devised by Page et al. (2002) 67. This tool utilized variables such as the amount of radiographical bone loss, tooth loss, furcation involvement and amount of calculus present at baseline. These variables were entered into the risk calculation. Other factors used to calculate risk were patient’s age, smoking activity, diabetic status and periodontal history. A risk score from 1 (low risk) to 5 (high risk) was calculated for each subject to determine the future prediction of periodontal status. The periodontal status in terms of alveolar bone loss (which utilized digital radiographs) and tooth loss (clinical records) was assessed at 3, 9 and 15 year. The authors used this risk assessment tool on 523 subjects enrolled in Veteran affairs dental longitudinal study to assess its validity. The results of the study suggested that risk scores ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
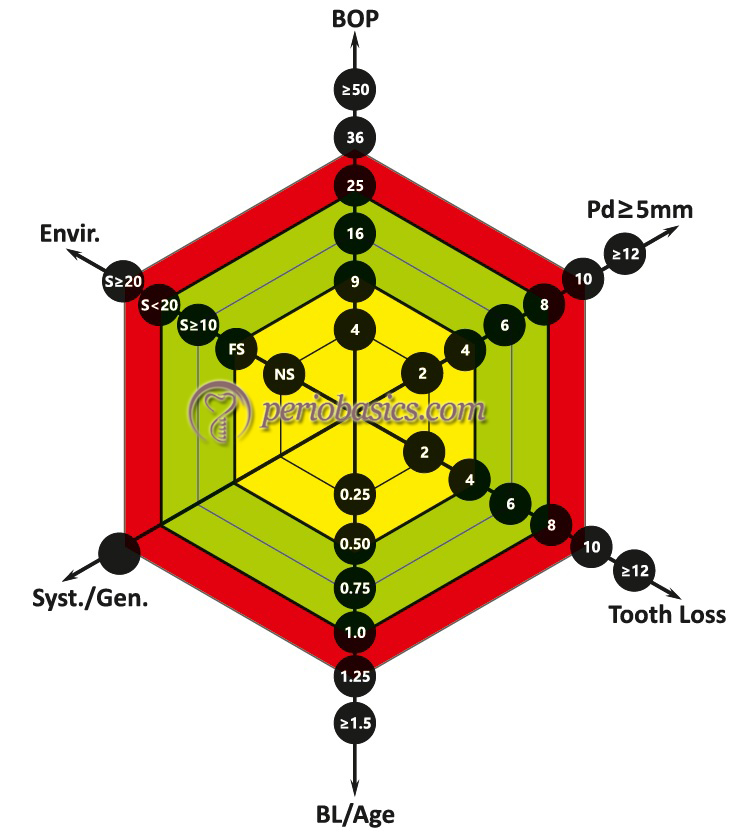
Lang and Tonetti (2003) 68 put forward a functional diagram to assess patient’s risk factors. In this diagram, authors suggested multiple clinical parameters, to determine the actual risk for a patient to develop periodontal disease. This is because of the reason that a single factor cannot be used as an accurate indicator of actual recurrence risk for periodontal disease. Multiple factors, when combined together, are more likely to give an accurate risk assessment for a particular patient. These factors include,
1. Percentage of bleeding on probing.
2. Prevalence of residual pockets greater than 4 mm (≥5 mm).
3. Loss of teeth from a total of 28 teeth.
4. Loss of periodontal support in relation to the patient’s age.
5. Systemic and genetic conditions.
6. Environmental factors such as cigarette smoking.
Let us discuss these factors,
Percentage of bleeding on probing:
Bleeding on probing (BOP) is one of the first signs of inflammation. It has been used as a good indicator of assessment of periodontal inflammation and has been incorporated into index systems for the evaluation of periodontal conditions 69, 70. BOP is also a good indicator for assessing patient’s self-performed plaque control abilities. Therefore, in the functional diagram of risk assessment, BOP has been considered as the first risk factor. It is expressed in percentage scale and runs in a quadratic mode with 4, 9, 16, 25, 36 and > 49% being the critical values on the vector. Although, there is no well-established level of BOP in overall dentition above which risk of disease recurrence can be established, but Lang and Tonetti in this functional ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Prevalence of residual pockets greater than 4 mm (≥5 mm):
The primary focus of active periodontal therapy in patients with periodontal pockets is the pocket elimination or reduction of pocket depth. The remaining pockets of ≥5 mm pocket depth indicate to some extent, the degree of success of periodontal treatment rendered. However, it cannot be considered as the sole parameter determining the periodontal status of a treated periodontal patient. When combined with BOP and/or suppuration, existing pockets are indicative of existing ecological niches from and in which re-infection might occur. Minimum remaining pockets following treatment are an indicator of periodontal stability and existence of deep periodontal pockets as well as deepening of periodontal pockets during periodontal maintenance are indicators of high risk for disease progression 57, 58. In the functional diagram, the pocket depths ≥5 mm have been considered as ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Loss of teeth from a total of 28 teeth:
The number of teeth present reflects the functional condition of the dentition. Loss of teeth due to any reason has an impact on the functional stability of the dentition. However, the mandibular stability can be assured with premolar to premolar occlusion even if some teeth are lost and the dental arch is shortened (20 teeth) 71, 72. Also shortened dental arch does not seem to predispose the individual to mandibular dysfunction 73-75. According to the authors, missing teeth are indicative of a patient’s history of oral diseases and trauma and therefore should be considered as a parameter for risk assessment. In the functional diagram ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Loss of periodontal support in relation to the patient’s age:
The alveolar bone loss in relation to patient’s age can be considered as the most obvious indicator of subject risk for disease recurrence. Our present understanding regarding periodontal disease progression suggests that both onset and the rate of progression of periodontitis might vary among individuals and during different timeframes 76. Also, previous bone loss in the patient does not rule out the possibility of the rapidly progressing lesions. The authors considered alveolar bone loss in relation to patient’s age as the fourth parameter for risk of disease recurrence in the functional diagram. Age has been considered as an important factor in risk assessment because, for similar bone loss in a young and an old individual, the young individual is at more risk for disease recurrence because of rapid disease progression as compared to the older patient. According to Papapanou et al. (1988), in treated patients, a reduced height of periodontal support (i.e. 25-50% of the root length) may be considered as a reliable prognostic indicator for the stability of the overall treatment goal of keeping a functional dentition for a lifetime 77.
In the proposed functional diagram, the bone loss estimation is done in the posterior region on periapical radiographs. Posterior sites have been chosen by the authors because they are more prone to bone loss. The bone loss at the worst site affected is grossly estimated in the percentage of root length. On bitewing radiographs, bone loss at the worst site affected is estimated in millimeters where 1 mm represents 10% of the bone loss. The percentage estimated is then divided by the age of the patient (BL/age). For example, for a 40-year old patient ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
In the functional diagram, the scale for BL/age runs with increments of 0.25 with 0.5 being the critical value to discriminate between low and moderate risk and 1.0 being the value for moderate and high risk.
Systemic and genetic conditions:
The relationship of systemic diseases such as diabetes mellitus with periodontal disease progression is well established. It has been shown that diabetes mellitus acts as a modifying factor favoring periodontal disease susceptibility and disease progression 78, 79. Another important factor is genetic susceptibility. Kornman et al. (1997) have demonstrated that IL-1 gene polymorphism is positively associated with advanced periodontal disease 80. Presently, various single nucleotide polymorphisms have been identified (TNF-α, IL-4, IL-6, IL-10, human Leukocytic Antigen polymorphism, Fc γ receptor (FcγR) gene ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Hence, systemic and genetic aspect has been considered as the fifth parameter for recurrent disease in the functional diagram of risk assessment. If these factor/factors are found to be present in the patient, the area of high risk is marked for this vector. If found absent, these factors are not considered as a component of risk assessment for disease recurrence.
Cigarette smoking:
Smoking is an important environmental factor involved in periodontal disease progression. Tobacco smoking rather than snuffing or chewing affects the susceptibility and the treatment outcome of patients with chronic periodontitis. Studies have demonstrated poor periodontal condition in patients who are tobacco smokers. Smoking has been positively associated with generalized forms of severe periodontitis in several studies 81-84. Although, BOP is reduced in smokers, but periodontal destruction is more as compared to non-smokers. In a study on healthy male Spanish military recruits, the clinical parameters to estimate the degree of periodontal disease were evaluated. The results revealed higher plaque and bleeding indices in non-smokers, although probing depths and attachment loss was greater in smokers 84. Another clinical study done in Northern Ireland demonstrated periodontal probing depth in excess of 4 mm was more than double in young smokers (15%) as compared to 6% in non-smokers 85. The periodontal ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Lang and Tonetti have considered smoking as the sixth risk factor for recurrent disease in the functional diagram of risk assessment. In this functional diagram, non-smokers, and former smokers are considered to have a relatively low risk for recurrence of periodontitis whereas heavy smokers (smoking more than one pack per day) are defined as a high-risk group. Occasional smokers (< 10 cigarettes a day) and moderate smokers (10-19 cigarettes a day) have been considered at moderate risk for disease progression.
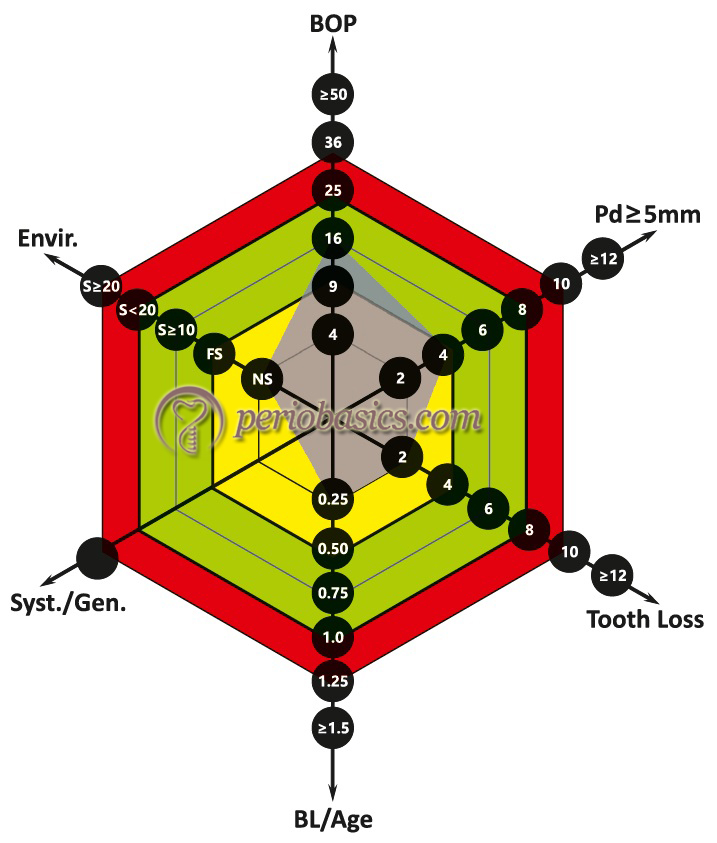
Patient’s individual periodontal risk assessment (PRA)
The authors have suggested that the individual risk assessment for a patient can be drawn in a functional diagram as shown in the above figures, Patients can be divided into low PRA, moderate PRA, and high PRA groups.
Low PRA patient:
In low PRA patients, all parameters are within the low-risk categories or at the most one parameter is in the moderate-risk category.
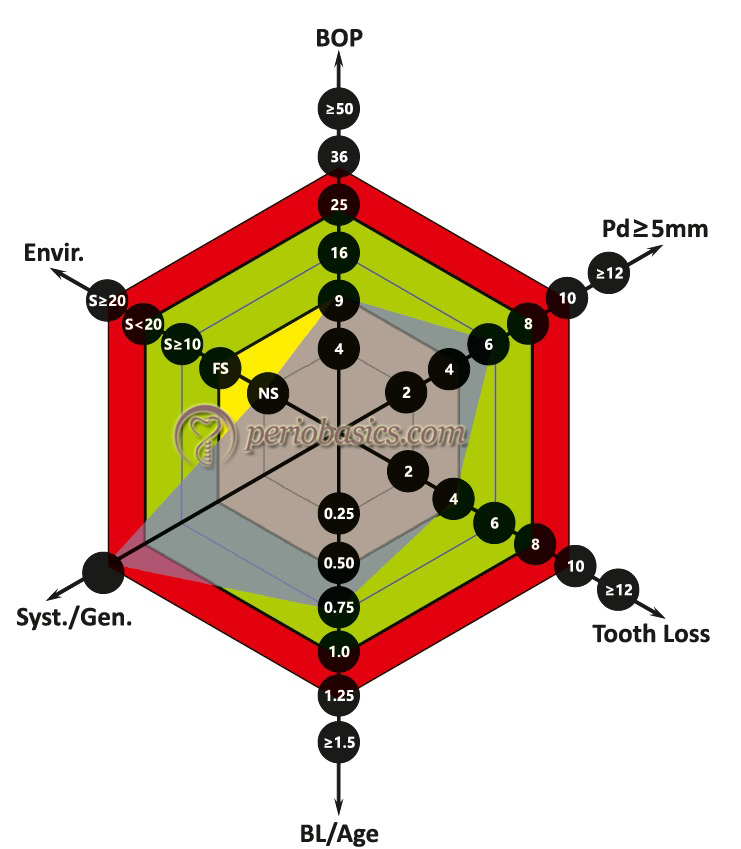
Moderate PRA patient:
Here, at least two parameters in the moderate category, but at the most one parameter in the high-risk category.
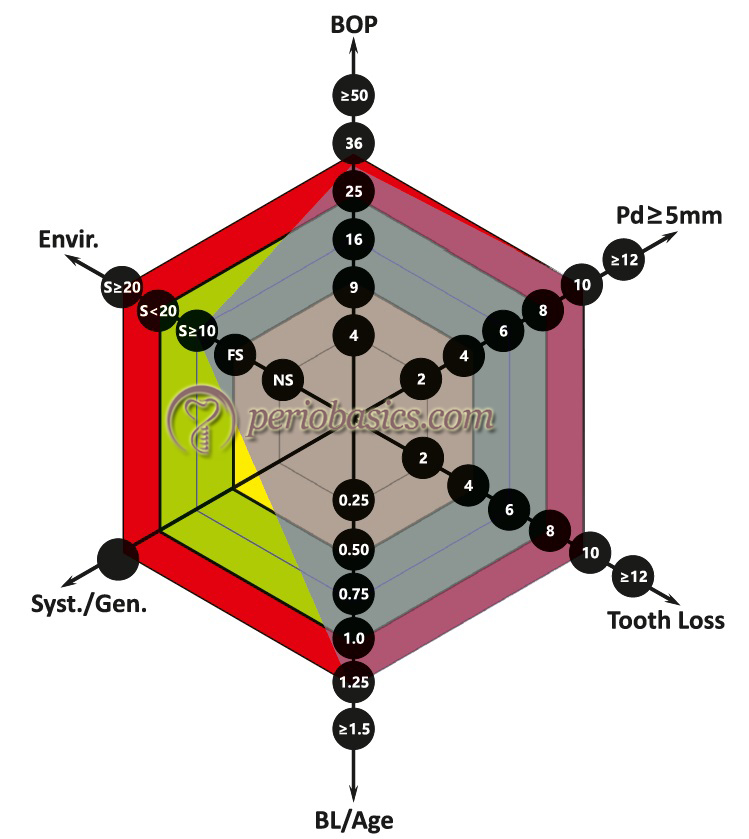
High PRA patient:
In these patients, at least two parameters are in the high-risk category. Out of all the parameters, BOP and residual pockets are easily affected by appropriate periodontal therapy, whereas others parameters, such as numbers of missing teeth or systemic and genetic factors are either irreversible and cannot be reduced or may only be affected to a great extent by the additional efforts (smoking cessation). The high-risk patients can be brought under the moderate risk category by appropriate periodontal treatment, thereby reducing BOP and remaining residual pockets.
Modified Periodontal Risk Assessment Model (Modified PRA)
Chandra (2007) 90, proposed a new periodontal risk assessment model which was based on the periodontal risk assessment (PRA) model by Lang and Tonetti (2003) 68. The modified PRA model is easier to generate and use. It assesses diabetes on an individual radius and also incorporates dental factors include “other factors” such as stress and socioeconomic factors. It has 4 factors of PRA model: BOP, the number of sites with pocket depth ≥5 mm, tooth loss and smoking. Additional factors which have been redefined or included are diabetic status, attachment loss (AL)/age, dental status-systemic factors interplay and other background characteristics. The main differences between PRA and modified PRA model are 91,
- Environmental factors, systemic and genetic factors are specifically defined as diabetes status and interplay of dental-systemic factors that accounts for dental factors.
- Bone loss/age is replaced with attachment level/age.
- Other background factors are included to include estimated socioeconomic or stress factors.
- Scores on each trajectory ranged between 1 and 5 based on a coding system rather than using actual factor thresholds such as BOP percent, or numbers of pockets ≥ 5 mm.
University of Ferrara (UniFe)
Trombelli et al. (2009) 92, proposed a new simplified method for periodontal risk assessment based on five parameters derived from patient’s medical history and clinical recordings. The five parameters included,
1. Smoking status,
2. Diabetic status,
3. Number of sites with probing depth ≥5 mm,
4. Bleeding on probing score (BOP) and
5. Bone loss/age.
Each parameter assessed is allocated a score. The algebraic sum of the parameter scores is calculated and relates to a risk score between 1 (lowest risk) to 5 (highest risk).
Dentition risk system (DRS) at both the patient and tooth level
Proposed by Lindskog et al. (2010) 93, it is a web-based analytic tool that calculates chronic periodontitis risk for the dentition (Level I) and for an individual tooth (Level II). The risk assessment is done on the basis of systemic and local predictors. The systemic predictors include age, family history of periodontitis, systemic disease, patient compliance and disease awareness, skin test result (assesses patient’s inflammatory reactivity), smoking habits, socioeconomic status ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Tooth risk assessment
Tooth positioning in dental arch:
Tooth positioning in dental arch may be considered as an important factor determining the periodontal health of teeth. An association of crowding with more plaque accumulation has been investigated by various researchers. Helm and Petersen (1989b) 94 and Gábris et al. (2006) 95 have shown a positive correlation between malocclusion and periodontal health, whereas Geiger et al. (1974) 96, Katz (1978) 97 and Buckley (1980) 98 found no association between the amount of plaque or periodontal parameters and malocclusion (including crowding and spacing). However, in one study Geiger (2001) 99 found a possible association between periodontal problems and certain malocclusions such as anterior overjet and overbite, crossbite etc. But, these cases were not particularly studied for plaque accumulation due to malocclusion.
The present evidence suggests that crowding may facilitate plaque accumulation in patients with irregular oral hygiene practices, but whether it results in increased risk of clinical attachment loss, remains to be investigated.
Residual alveolar bone support:
The residual alveolar bone support is an important risk factor for tooth loss due to further bone loss. It has been shown by various studies that teeth with reduced periodontal support, but healthy periodontium can function for several years either individually or as abutment provided that the occlusal load does not cause trauma to the periodontium 100-102. However, if the periodontal ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Mobility:
Increased tooth mobility indicates two probable reasons: loss of periodontal support or increased occlusal load. A progressive increase in tooth mobility indicates of these two underlying causes. Another important factor to be considered here is crown root ratio. An increased crown root ratio results in increased lateral tooth mobility. However, it must be noted that the periodontal status of a tooth cannot be assessed only on the basis of tooth mobility. It has been demonstrated by various studies that tooth mobility may vary before, during and after periodontal treatment 103, 104. After non-surgical and surgical periodontal therapy, the tooth mobility is usually reduced. However, tooth mobility may temporarily increase following surgical periodontal therapy during the healing period and may gradually reduce later on.
Iatrogenic factors:
The common iatrogenic factors responsible for periodontal disease recurrence are overhanging restorations and ill-fitting crown margins. The association of subgingival plaque retentive factors and development of periodontitis is well documented [for more, see review by Leon (1977) 105]. The constant presence of plaque in subgingival areas such the under the margins of subgingival restorations has been shown to change the ecological ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Site risk assessment
Bleeding on probing:
BOP is a reliable clinical sign of periodontal condition and disease progression 107. Lang et al. (1990) 108 have demonstrated that absence of BOP represents a reliable indicator of periodontal stability. It has also been shown that sites with overt gingival inflammation show more disease progression as compared to sites without inflammation 109. Lang et al. (1991) 110, demonstrated almost a linear relationship between probing force and percentage of sites that bleed on probing. The authors suggested a probing force of 0.25 N (25 gm) to assess BOP without provoking bleeding by causing gingival trauma. 0.25 N is a light force which induces bleeding only from the inflamed gingiva. However, the standardization of the probing force should be done before probing. The pressure-sensitive probes have been designed to ensure a constant probing force during probing (for more, read “Periodontal instruments”).
During every periodontal maintenance visit, sites with BOP should be registered. A constant force of 0.25 N should be used to probe all the sites. Sites which demonstrate BOP frequently during maintenance visits ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Clinical attachment loss:
Clinical attachment loss is indicative of periodontitis. It is clinically measured as the distance of the epithelial attachment from the cementoenamel junction which is the normal site for epithelial attachment. The most accurate method for establishing attachment loss is no doubt histological analysis. However, clinically it can be measured with the use of graduated periodontal probes. Various factors that may affect the measurement of the attachment loss clinically are probe dimension, probing force, the direction of probe placement and condition of the gingival tissue. The presence of calculus at the cementoenamel junction may lead to the inaccurate recording of attachment loss. Therefore, calculus and other deposits should be removed, followed by the recording of attachment levels. After periodontal therapy, once healing is complete, first reading should be considered as the baseline for long-term clinical monitoring 111.
The ideal outcome of non-surgical and surgical periodontal treatment is the ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Suppuration:
The active periodontal disease results in disease activity in the periodontal pocket, which may result in abscess formation which may drain through the pocket orifice. It has been shown that suppuration is an indicator of future loss of attachment 48, 57, 58. Suppuration along with other parameters such as BOP and increased probing depth is positively related to the future periodontal breakdown.
Clinical implementation of multilevel risk assessment
After the patient has been assessed for a person-based, tooth based and site based risk assessment, a combination of these parameters can be used as a guide to determine the overall risk profile of the patient and to plan the maintenance therapy for the patient. Multilevel risk assessment helps in more accurate planning of the maintenance therapy for a patient as compared to single-level risk assessment because it allows the assessment of the influence of patient-based factors such as smoking, diabetes etc. on periodontal disease recurrence. The multi-level risk assessment also helps in more accurate determination of recall frequency and time requirements.
Establishment of maintenance intervals
Many studies have been done to determine the best time interval between the maintenance visits so that an optimum periodontal health of the patient can be achieved. Time interval varying from 2 weeks 4, 3 months 19 to 4-6 months 16 have been suggested. However, it must be understood that the periodontal maintenance visits should be scheduled based on individual risk assessment for recurrence of the disease 112. The Merin’s classification system is widely used for patient recall following the active periodontal treatment.
Merin’s classification
In this classification system, during the first year following treatment, the patient is scheduled for periodontal maintenance visits at 1-2 months or 3 months intervals depending on healing following treatment and complexity of the case. After 1 year, the patient is classified into class A, B or C depending on whether the results of the periodontal treatment are maintained well or not during the first post-operative year, other complexities in case, environmental factors like smoking and systemic diseases which contribute to periodontal disease progression.
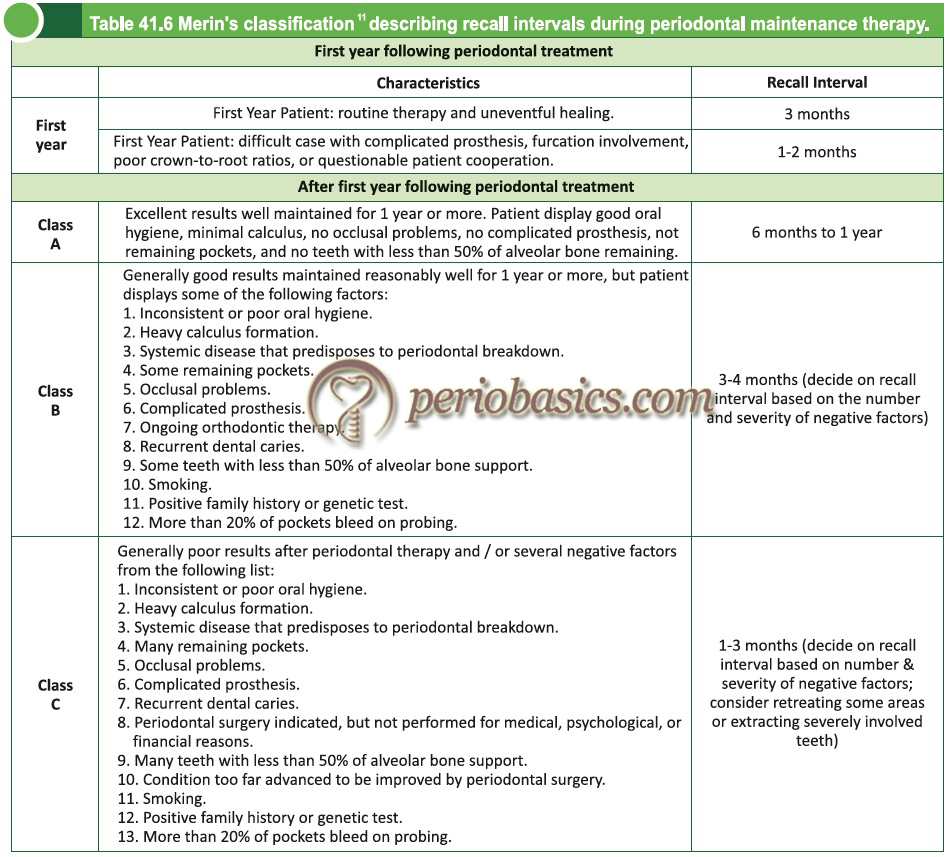
The first year following periodontal treatment is more critical in terms of motivating the patient to participate in the recall periodontal maintenance program and also to reinforce the oral hygiene techniques used by the patient. Furthermore, the results of the surgical periodontal therapy can only be evaluated accurately several months following the ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
As already stated, after one year the patient is classified into class A, B or C. According to the improvement or deterioration of the periodontal status of the patient, the class where the patient fits in, may change. In the case where one dental arch is involved more than the other dental arch, patient’s periodontal condition is classified by the arch which is in worse condition.
Patient attendance compliance
Compliance is defined as ”the extent to which a person’s behavior coincides with medical or health advice” 114. As can be expected, highly compliant patient has been shown to have better periodontal prognosis as compared to non-compliant patients. The first study to check patient compliance was done by Wilson et al. (1984) 115 who assessed the degree of compliance of 961 patients who were followed for up to eight years. The results of the study showed that only 16% of the patients completely complied with periodontal maintenance therapy intervals, 34% never returned for periodontal maintenance therapy, and the rest complied erratically. In a follow-up study, the same patients were followed up for five years to assess tooth loss. It was observed that erratic compliant had 14% tooth loss (0.06 per patient per year) whereas none of the complete compliers lost teeth. Many other ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
There are multiple and complex reasons for non-compliance of patients, which may vary from patient to patient. The most common reasons for noncompliance include personal reasons, economic reasons, psychological reasons and mere ignorance. It has been found that most of the non-compliant patients have more stressful life events and less secure personal relationships 121. These findings have suggested that dentist may be helpful in modifying these underlying causes, but to what extent is still debatable. However, it has been observed that behavioral management can provide positive reinforcement and may significantly improve the patient compliance 122. These findings have been supported by another study, which ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
It has been suggested that patient must be told at the onset of periodontal treatment that the long-term success of the treatment will depend on the willingness of the patient to adhere to a well scheduled periodontal maintenance therapy program.
Components of a periodontal maintenance visit
According to the American Academy of Periodontology (2011) 124, a periodontal maintenance visit should include,
- Update of medical and dental histories.
- Evaluation of current extra- and intraoral periodontal and peri-implant soft tissues as well as dental hard tissues and referral when indicated (e.g., for the treatment of carious lesions, pulpal pathosis, or other conditions) and diagno-stic quality radiographs when appropriate.
- Assessment of the oral hygiene status with re-instruction when indicated.
- Mechanical tooth cleaning to disrupt/remove dental plaque, biofilms, stain, and calculus. Local or systemic delivery of chemotherapeutic agents may be used as adjunctive treatment for the recurrent or refractory disease.
- Ongoing assessment of risk factors to identify an individual who may be more highly susceptible to ongoing breakdown of the periodontal or peri-implant tissues, with elimination or mitigation of new or persistent risk and etiologic factors with appropriate treatment.
- Identification and treatment of new, recurrent, or refractory areas of periodontal and peri-implant pathoses.
- Establishment of an appropriate interval for periodontal maintenance.
The patient should be kept informed of:
- Areas of persistent, recurrent, refractory, or newly occurring periodontal or peri-implant disease.
- Changes in the periodontal prognosis and risk factors associated with periodontal diseases.
- Advisability of further periodontal treatment or re-treatment of indicated sites.
- Status of dental implants.
- Other oral health problems that may include caries, defective restorations, and non-periodontal mucosal diseases or conditions.
- Changes that would warrant a referral to, or consultation with, other dental or medical specialists.
Protocol for periodontal maintenance visit:
Periodontal maintenance therapy consists of an orderly sequence of procedures which are carried out to accurately assess the present medical and dental status of the patient.
Examination and re-evaluation of the patient and diagnosis:
The first and foremost step is to re-evaluate patient’s current medical and dental health status and risk factors. The information obtained is essential to determine the periodontal diagnosis and prognosis of the dentition and/or the suitability of dental implants. If the patient has any chief complaint, it is recorded and medical or dental history is reviewed. A detailed clinical examination is done, followed by radiographical analysis. Microbiological, genetic, biochemical, or other diagnostic tests may also be useful, on an individual basis, for assessing the periodontal status of selected individuals or sites. The following steps are followed during a comprehensive periodontal evaluation:
- Extra-oral and intra-oral examination to detect any non-periodontal disease or condition.
- Intra-oral hard tissue and soft tissue examination is done. The teeth are examined for the presence of caries, proximal contact relationships, status of dental restorations and prosthetic appliances, and tooth- or implant-related problems. The periodontal examination includes measurement and recording of probing depths, the width of keratinized tissue, gingival recession, and attachment level. Sites with BOP/suppuration are recorded which indicate re-infection. Furcation status of the posterior teeth is evaluated. Any endo-perio lesion if present, is identified. The status of dental implants and their surrounding tissue is evaluated.
- The present status of presence and distribution of plaque biofilm, calculus, and inflammation of soft tissue is evaluated and recorded using suitable indices.
- The occlusal stability is re-evaluated by assessing occlusal patterns and discrepancy, determining the degree of tooth mobility, determination of fremitus and occlusion associated with implants.
- A radiographic examination is done to evaluate the current status of bone support surrounding the teeth and implants, including the bone quality/quantity and establishment bone loss pattern.
- Assessment to evaluate the need and suitability of dental implants.
- Re-evaluation of risk factors associated with the patient such as age, smoking, diabetes, cardiovascular disease, and any other systemic conditions which may affect the periodontal disease progression.
Using multi-level risk assessment, the overall risk status of the patient is determined and an appropriate treatment plan is established.
Patient motivation and re-instructions:
One of the most important steps during a periodontal maintenance visit is patient motivation as it affects compliance and home care of a patient. Many patients think that the active phase of the periodontal treatment is “cure” for their periodontal problems and express surprise at the need for further treatment of recurrent disease, or the need to attend recall visits during maintenance therapy. A good communication between the dentist and patient should be established to explain the patient the importance of periodontal maintenance therapy. Patient motivation should be based on the individual needs of a patient. Some patients may present with wear facets at the cervical regions of teeth, which indicates overzealous and/or faulty tooth brushing. These patients should be ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Treatment during a maintenance visit:
The treatment during a maintenance visit primarily involves scaling and root planing (SRP) and treatment of re-infected sites. It has been recommended that instead of the instrumentation of all the tooth surfaces, only those sites, which exhibit signs of inflammation and /or active disease progression should be treated by SRP. All the sites with BOP and probing depth exceeding 5 mm are carefully re-scaled and root planed. If re-instrumentation is done at healthy sites, it may result in further attachment loss 125. In an article on “Critical probing depth”, Lindhe et al. (1982b) 126 demonstrated that the instrumentation of pockets below 2.9 mm may result in attachment loss and designated it as critical probing depth below which instrumentation should not be done.
The sites which are re-infected should be given particular attention during the maintenance visits. The most common causes of re-infection are incomplete instrumentation during active periodontal treatment and inadequate plaque control by the patient. The re-infected sites may exhibit suppuration and are treated by thorough instrumentation under anesthesia. In certain cases, surgical access may be required for appropriate debridement of the re-infected area. Treatment modalities such as ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Following the completion of the recommended treatment, polishing of the entire dentition is done so there are no deposits on the tooth surface and tooth surfaces are free of any stains and are smooth. Following polishing, fluorides should be applied on teeth so the lost fluorides during instrumentation can be compensated. In areas of recession fluoride varnishes or chlorhexidine varnishes should be applied to prevent root surface caries.
Determination of patient recall interval:
The last step during a periodontal maintenance visit is to determine the recall interval for the next visit. This can be done by establishing the overall patient risk by assessing the multi-level risk assessment of the patient. Merin’s classification is also helpful in determining the recall intervals during periodontal maintenance therapy.
Dental implant maintenance
Dental implants have been widely used as a successful alternative to fixed and removable prosthodontic restorations 128, 129. The long-term success of dental implants primarily depends on the maintenance of a healthy peri-implant soft tissue. The inflammation in the peri-implant soft tissue results in progressive bone loss around the crestal portion of the implant, which may ultimately result in the implant mobility and implant failure. Dental implant health is evaluated ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
It must be noted that except for certain differences like lack of periodontal ligament, the orientation of collagen fibers and biological width; peri-implant tissue and periodontal tissue have many similarities 130, 131. The plastic body periodontal probes are widely used for the assessment of peri-implant tissue. However, the diagnostic value of probing around dental implants remains controversial 132, 133. The most effective way of assessing bone loss around dental implants is conventional or digital subtraction radiography. A vertical bone loss less than 1.5 mm during the first year and 0.2 mm every subsequent year has been offered as the criterion for the clinical success of dental implants 134.
During periodontal maintenance, our primary goals to maintain implant health are,
- Prevention of plaque formation around implant,
- Inhibition of early plaque maturation,
- Elimination of the existing plaque, and
- Elimination of occlusal abnormalities associated with implant abutment.
Application of metallic instruments on dental implant surface damages the surface properties of the dental implant. It has been observed that ultrasonic scaling with metallic tips may severely disrupt the titanium dioxide layer and may result in the formation of plaque retentive areas on the implant surface. In one study Rapley et al. (1990) 135 evaluated the effects of various oral prophylactic materials, including rubber cup, rubber cup with flour of pumice, air abrasive, interdental tapered brush, Eva yellow plastic tip, soft nylon toothbrush, universal plastic scaler, ultrasonic scaler and stainless steel scaler on titanium abutments. On viewing under an electron microscope, it was observed that metal sealers produced significant vertical grooving on titanium surface, whereas instrumentation with the interdental brush, Eva plastic tip, rubber cup, air abrasive, soft nylon ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Studies have been done to find out the effectiveness of various subgingival anti-microbial irrigation solutions in reducing peri-implant inflammation and reducing microbial load. In a study, Listerine was used around the dental implant as a subgingival irrigation solution and its effect in plaque reduction and inflammation reduction was evaluated. Results demonstrated a significant reduction in plaque index, gingival index and bleeding index with no significant reduction in probing depth 136. On the other hand, one study found ……… Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Conclusion
Periodontal maintenance therapy is an integral part of complete periodontal treatment. During the maintenance phase of periodontal therapy, the clinician can re-evaluate the patient and modify treatment according to the presence of risk factors. The most important part of maintenance therapy is patient motivation. Patient’s compliance can be improved by repeated counseling of the patient. With an appropriately planned periodontal maintenance therapy and adequate home care by the patient, post-treatment periodontal and peri-implant health can be maintained for the lifetime of the patient.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.