Introduction to occlusal trauma
Occlusal trauma is detrimental to periodontal health. It may act as a cofactor which can increase the rate of progression of an existing periodontal disease. Thus, elimination of occlusal trauma is essential to achieve complete periodontal health. The first and foremost principle for the initial treatment of patients diagnosed with periodontitis with slow, moderate or rapid rate of disease progression in which the etiologic factors are both bacterial plaque and occlusal factors, is to eliminate and control first the plaque and then the occlusal factors, except where delay may unfavorably influence treatment of occlusal abnormalities, or cause discomfort to the patient. The end point of the occlusal therapy should be to achieve stable occlusion with the least interference to plaque control and periodontal maintenance. The following treatment modalities can be used to treat the occlusal abnormalities as a part of periodontal treatment,
- Orthodontic treatment.
- Splinting.
- Restorative treatment.
- Occlusal adjustment.
Orthodontic treatment
It is an established fact that there is no significant relationship between malocclusion and severity of the periodontal disease. So, orthodontic treatment should not be considered as a routine treatment for preventing or treating periodontitis. However, there are specific situations where orthodontic treatment is essential to achieve optimal results of periodontal therapy. In the following situations, orthodontic treatment becomes essential to achieve periodontal health,
- Impinging overbite where trauma to gingival tissue is causing gingival recession. In extreme cases, a combination of orthodontic and surgical procedures may be required.
- Lack of lip seal and mouth breather’s gingivitis may indicate the need for orthodontic treatment.
- Up-righting of tipped teeth helps in reducing periodontal pocket depth as well as facilitate restorative treatment and plaque control.
- Presence of anterior cross-bite is an important indication for orthodontic treatment. It is accompanied by an unstable jiggling type of occlusion, which seems to aggravate periodontitis.
- Extensive open bite with contacts only on the last molars often has associated periodontal problems and orthodontic treatment may be beneficial.
- Correction of severely malpositioned teeth improves the long-term prognosis of the dentition.
- Orthodontic intrusion of anterior teeth with advanced periodontal destruction may help in improving their periodontal support.
It must be noted here that, orthodontic treatment should be done only when inflammation in periodontal tissues has subsided following scaling and root planing and the patient is maintaining good oral hygiene. Tooth movement in the presence of gingival inflammation may be detrimental.
Splinting
It is a procedure by which the resistance of a tooth to the occlusal forces is increased by joining a neighboring tooth or teeth. It is a well-accepted treatment used to control irreversible tooth mobility through mechanical stabilization. It stabilizes the mobile teeth by forming a firm unit, thus minimizing tooth mobility and greatly improving the occlusal function of teeth. It not only ensures the retention of the periodontally compromised teeth, but also positively affects their longevity in the oral cavity. Splinting may be done for short term or long term. The primary objective of splinting is to ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Restorative treatment
Restorative treatment is sometimes essential to achieve periodontal health. Food impaction, impinging overbite or various forms of unstable occlusion require restorative treatment. Permanent splints are also a component of restorative treatment. It should be noted here that permanent splinting of teeth should be considered only after other forms of occlusal therapy have been ruled out as being inadequate.
Occlusal adjustments
In order to have a healthy masticatory system, periodontal trauma because of faulty occlusion should be treated. A successful adjustment in the occlusal abnormalities results in occlusal stability. Occlusal adjustment may also eliminate food impaction and gingival impingement in some instances. It should be remembered that because occlusal adjustment involves removal of tooth structure and is an irreversible treatment, it should be carried out only after a definite diagnosis has been made regarding the presence of a traumatic lesion rather than the presence of any occlusal interferences, which may be ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
In the following paragraphs, we shall read about the occlusal adjustment,
Indications for occlusal adjustment
It must be remembered that occlusal adjustments result in changes in occlusal scheme. It is an irreversible treatment so should only be planned with great care. Even minor mistakes made during the occlusal adjustment may result in worsening of the situation. Following are the indications for occlusal adjustment,
- The presence of parafunctional habits in conjunction with occlusal disharmony.
- Signs of occlusal trauma, excessive occlusal attrition, and/or TMJ dysfunction.
- The presence of multiple restorations on posterior or anterior teeth, which require occlusal adjustment to achieve a harmonious occlusion.
- To eliminate occlusal interferences after the orthodontic treatment is finished.
- Some clinicians also recommend prophylactic occlusal adjustments in the absence of any periodontal or TMJ symptom to prevent future problems.
Evaluation of TMJ and occlusion
A precise occlusal history should be recorded before any occlusal examination is done. The details of the history depend on the type of occlusal symptoms and their severity. The patient’s problems and their duration should be recorded in a chronological order. The patients usually cannot relate the occlusal problems with their symptoms. So, appropriate questions should be asked to establish any relation between the patient’s symptoms and occlusal abnormalities. Para-functional habits are the most common cause of occlusal problems. So, the patient should be asked questions about the history of pain in teeth, periodontium or TMJ and associated musculature.
The patient should be asked questions like: “Do you have your teeth in tight contact when you wake up? Do you feel tiredness in the jaws on waking up?” Any positive answer indicates parafunctional habit. The patients usually do not know about night grinding. So, any other person sleeping with the patient should be asked about ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Extra-oral examination
The patient should be made to sit in a semi-recline position with head slightly tipped back. The head should be supported by the headrest. Any facial asymmetry should be noted and the cause of abnormality should be detected. The patient should be asked to open and close the mouth slowly. Any deviation during mouth opening or closing should be noted. The TMJ examination should be done by lateral palpation of the joint and auscultation of the joint should be done (For more detail, “Art of history taking in periodontics”). The muscles of mastication should be palpated for any tenderness.
Intra-oral examination
The intra-oral examination of the patient should be done to identify any occlusal interference. It must be emphasized here that any single positive sign should not be considered as diagnostic of the occlusal problem, but should be related carefully to other findings. The following steps are followed while recording functional occlusion,
- The static relation between maxillary and mandibular teeth i.e., centric occlusion (CO) position should be determined first.
- Overjet, overbite and freeway space should be determined.
- Any occlusal variation in the occlusion plane, cross-bite, open bite, extrusion etc. should be recorded.
- Wear facets and their distribution should be recorded. It should be remembered that the presence of wear facets is related to patient’s age.
- The presence of wear facets is not always pathognomonic of traumatic occlusion. So, it must be correlated with other findings.
- Tooth/teeth with increased mobility should be identified. Along with increased tooth mobility, increased tooth sensitivity to thermal changes and to percussion should also be checked because these findings can also be due to occlusal trauma.
- Any tooth migration should be recorded. Tooth migration associated with an occlusal abnormality is usually associated with wear facet.
- Tooth migration without wear facets is usually associated with abnormal tongue habits or atypical swallowing habits.
- Radiographic examination of teeth with mobility or migration should be done. Loss of bone support or changes in periodontal ligament space are indicative of trauma from occlusion.
Diagnosis of occlusal interferences
An “occlusal interference” is any tooth contact that inhibits the remaining occluding surfaces from achieving stable and harmonious contacts 15. Very small interferences up to 15 µm can trigger an untoward response such as tooth pain or mobility 16, 17. Hence, these interferences must be eliminated to achieve a stable and harmonious occlusion. In a harmonious occlusion without any interference, the occlusal contact time simultaneity, by definition implies that a time of 0 seconds elapses between the first and the last occlusal contact 18. In other words, we can say that all the occluding surfaces of the mandibular teeth come in contact with the maxillary teeth at the same instant during the mandibular closure.
There are four types of occlusal interferences:
- Centric.
- Non-working.
- Working.
- Protrusive.
Armamentarium required for diagnosing and correcting occlusal interferences
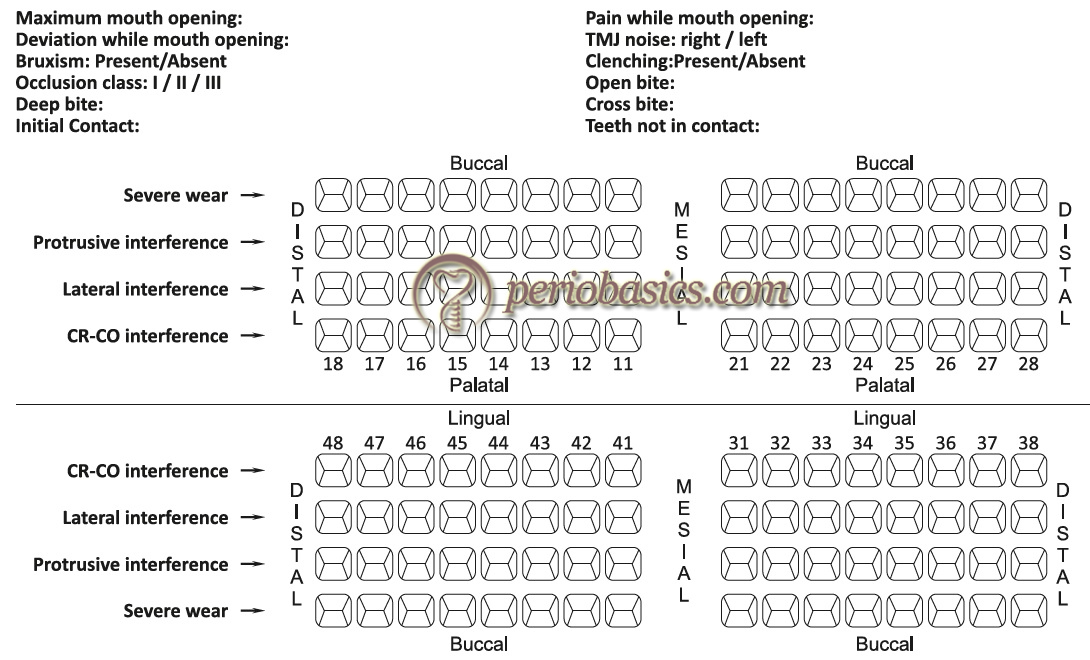
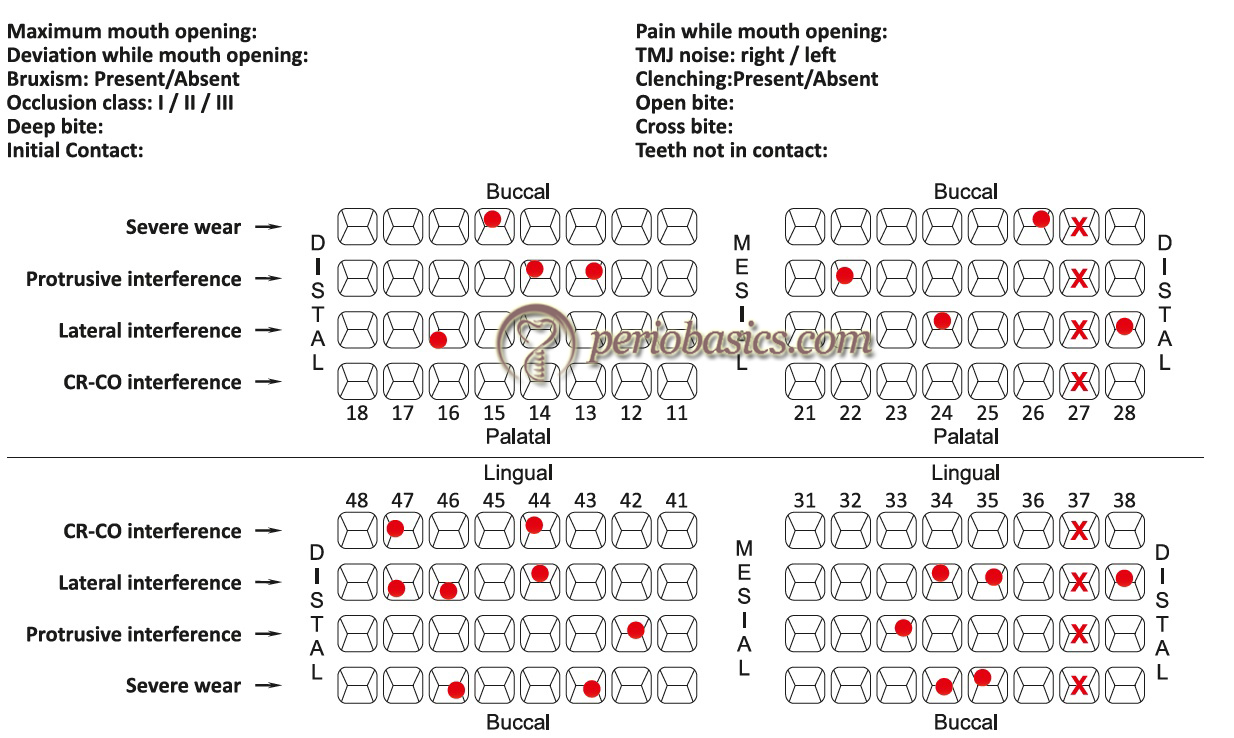
The armamentarium used to record functional occlusion includes occlusal indicators (described below), cotton rolls, dental mirror, hand mirror, abrasive disks and wheels, cutting and abrasive burs, polishing burs and rubber polishing cones. The findings of the occlusal examination should be recorded on a chart which consists of columns for recording all the significant occlusal parameters.
Occlusal indicators are essential components of recording functional occlusion. Occlusal indicators can be divided as qualitative and quantitative indicators. The primary difference between the qualitative and quantitative indicators is that quantitative indicators are capable of recording the tooth contact events.
Qualitative indicators:
- Articulating paper.
- Articulating silk.
- Articulating film.
- Waxes.
- Metallic shim stock film.
- High spot indicator.
Quantitative indicators
- T-Scan occlusal analysis system.
- Virtual dental patient.
Qualitative indicators
Articulating papers:
Articulating papers are the most commonly used occlusal indicators. These consist of a coloring agent and a bonding agent between the two layers of the film. On making tooth contact, the coloring agent is expelled from the film and the bonding agent binds it onto the tooth surface. In areas with heavy contact, the dye spreads peripheral to the actual location of the occlusal contact making a central area that is devoid of the colorant surrounded by a peripheral rim of the dye. The central area of the contact indicates interference and requires correction. Articulating papers are available with different width, thickness and ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..

Articulating silk:
A better way to avoid pseudo-markings is to use an articulating silk. It is made up of micronized color pigment, embedded in a wax-oil emulsion. However, it should be remembered that its marking capability is lost if the staining components are dried. Secondly, contamination of the field by saliva spoils the markings. Hence, it should be used in a dry field and should be stored in a cool and closed environment. It can be used on highly polished surfaces which is its important advantage over articulating papers.
Articulating films:
These are made up of emulsion ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Waxes:
Thin sheets of dark-colored wax are available which can be placed over the occlusal surfaces of the teeth in one arch. The opposing teeth are tapped gently into the wax until it perforates. The perforation represents interfering contacts. These are then marked with pencil and reduced. Waxes are very useful in identifying interferences on sharp line angles.
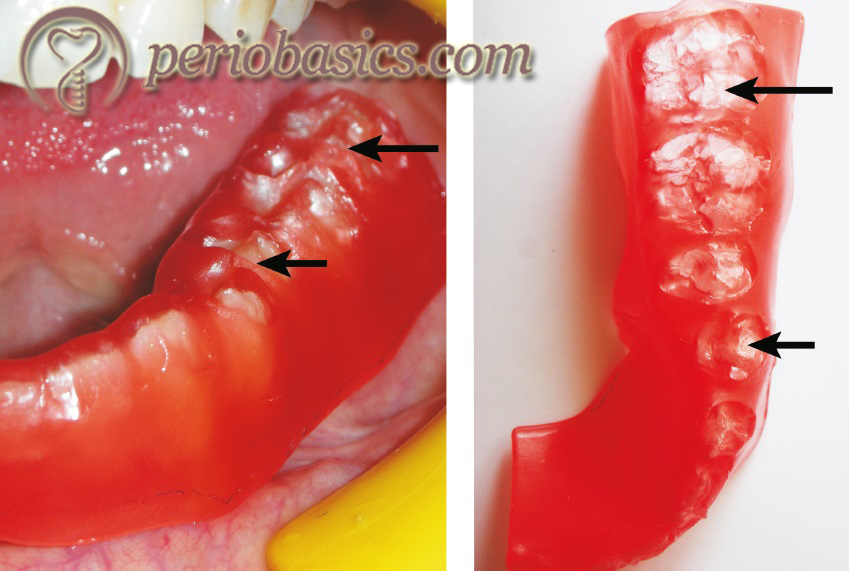
Metallic shim stock films:
These contain metallic surface on one side and coloring agent on the other side of the film. These are primarily used to accurately mark the contacts on the soft splint.
High spot indicators:
These are also used in the laboratory to check the proximal contacts of crowns, inlays, onlays, telescopic crowns and clasps. These are supplied in the form of a liquid which is applied over the proximal areas where it forms a thickness of 3 µm.
Quantitative indicators:
T-Scan occlusal analysis system:
This is a quantitative indicator which provides contact sequence in 0.01 second increments. The main advantage of this scan is that it identifies time magnitude along with the distribution of the occlusal contacts. The device consists of a piezoelectric foil sensor, a sensor handle and software and hardware to record the data. The foil sensor is placed between the maxillary and mandibular arches and an arch support is placed between the maxillary central incisors of the patient. After the recording button is pressed, the patient is asked to close his/her mouth slowly in the maximum intercuspation position without making any lateral movement.
The sequence of ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Virtual dental patient:
This is a recently introduced technology wherein patient’s dentition casts are scanned and a three-dimensional virtual occlusion is established. The functional movements on this virtual model provide us the quantitative information regarding the occlusal interferences. Similar to the T-scan, the sequence of the occlusal contacts, enables us to eliminate the initial contacts and hence the interferences.
Determination and recording of CR and CO position
The patient should be seated in a reclined and comfortable position in the dental chair with the head properly supported by the headrest. The patient should be asked to take a deep breath and relax the body as much as possible. The patient is asked to look in front and to keep the head stable during manipulation of the lower jaw.
Now, the little finger is placed slightly behind the angle of the jaw and remaining three fingers on the border of the mandible. The thumb is placed over the notch over the sym-physis. The patient is asked to open and close the mouth and the hinge movement of the mandible is felt. A firm pressure is then applied with fingers in an upward direction and with the thumb in a downward and backward direction to position the condyle of the mandible in terminal hinge position. It must be made sure that the manipulation of the mandible in the terminal hinge position should be totally free of any muscular influence. The position is then again verified by repeating the procedure. While the terminal hinge position is verified repeatedly, the patient is asked to gently close the mouth.
Sometimes, the patient complains of pain or discomfort while positioning the mandible in terminal hinge position. It indicates that the condyle meniscus assembly has not been braced against the bone. In such a situation repositioning of the mandible is done by placing cotton rolls between anterior teeth or by placing Hawley’s bite plane.
Once the CR position is well established, an articulating paper (preferably blue) is placed with the help of Miller’s forceps between the occlusal surfaces of teeth on the side making initial contacts. To avoid pseudo markings, thin articulating paper such as GHM occlusion foil (Hanel-GMH Dental GMBH, Nurtingen, Germany) which has 19 μm thickness should be used. The patient is then asked to slowly close the mouth to make contact of maxillary and mandibular teeth. The pair of teeth, making initial ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Registration of lateral and protrusive excursions
The lateral excursive movements are preferably recorded with a different color (such as red) than used for recording CR and CO. A dental tape is placed between the teeth of the patient on the right side and with the help of hand pressure mandible is moved to the right. Teeth with red marks are recorded on the occlusal chart. A similar procedure is then repeated on the left side and markings are recorded on the occlusal chart. A hand mirror can be given to the patient if he/she faces difficulty in performing lateral excursions. The protrusive excursion movements are recorded by gliding the teeth forward from the CO position without any lateral movement.
Now, the dental tape used to record CO and CR position is placed between the teeth and the patient is asked to bring teeth in CO position. The CO points of contact will superimpose on the lateral and protrusive contacts. The CO contact points (blue) can be differentiated from the lateral contacts (red) by their color difference.
Impression making and articulator analysis
Although the information gathered from contact point markings in CR, CO, lateral and protrusive positions are sufficient to identify the occlusal interferences; but for accurate diagnosis and treatment planning, the impressions are ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Types of occlusal therapy
Occlusal therapy is any treatment that alters a patient’s occlusal condition. It can be used to improve the function of the masticatory system through the influence of occlusal contact patterns and by altering the functional jaw position. Occlusal therapy can be reversible or irreversible. Reversible therapy temporarily alters the occlusal condition, the joint position, or both. The example of this therapy is occlusal splints. The disadvantage of reversible occlusal therapy is that the original condition might return after the therapy is discontinued. On the other hand, irreversible therapy permanently alters the occlusal condition so that the original condition cannot be recovered. The examples of irreversible occlusal therapy include selective grinding, fixed prosthetic procedures, and orthodontic therapy. In the following sections, we shall discuss in detail the irreversible occlusal therapy (selective occlusal grinding).
Principles of selective grinding
The clinical procedure to eliminate occlusal interferences consists of three procedures, namely grooving, spheroiding and pointing 19. Grooving is done to re-establish the depth of developmental grooves. Spheroiding is done to restore the original tooth contour in areas with supra-contacts. Once the supra-contacts have been identified, the burs are applied with a paint brush like manner over the markings and reshaping is done up to 2-3 mm mesially and distally from the marking and 2-3 mm apical to the marking. The cusp height should be maintained during this procedure. In situations where ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Steps in the correction of occlusal interferences
Once the occlusal interferences have been identified, the clinician must determine the extent of occlusal adjustments required. As already stated, these adjustments should be first performed on the articulated casts and then should be duplicated on the patient. Another important factor to be considered while doing occlusal adjustment is the age of the patient. In younger patients, usually conservative approach is adopted because they have a developing dentition which may have many unpredictable mechanisms for occlusal harmonization. Only minor occlusal adjustment, interceptive in nature is adopted in these patients. On the other hand, in older patients extensive occlusal adjustment can be planned.
Basic principles followed to eliminate occlusal interferences
The selective occlusal grinding is done to eliminate the occlusal interferences in a stepwise manner. These are,
Step 1: Elimination of retrusive supra-contacts and deflective occlusal interferences from CR to CO.
Step 2: Adjust CO to achieve stable, simultaneous, multi-pointed, widely distributed contacts. The unbalanced cuspal inclines and contacts should be eliminated to maintain or move the force vectors along the long axis of the tooth.
Step 3: Test for excessive contact (fremitus) on the incisal teeth.
Step 4: Remove posterior protrusive supra-contacts and establish contacts that are bilaterally distributed on the anterior teeth.
Step 5: Remove all interferences to lateral excursions.
Step 6: Eliminate gross occlusal disharmonies. Improve the occlusal anatomy by maintaining the cusp form, by creating correct marginal ridge relationships, cusp-fossa relationships, elimination of broad facets and narrow occlusal tables.
Step 7: Re-check tooth contact relationships.
Step 8: Polish all rough tooth surfaces.
Following is the detailed description of these steps,
Step 1:
The first step in the elimination of occlusal interferences is to remove these interferences in retrusive and CR to CO position. The primary objective here is to remove the supra-contacts and remove interferences that interfere with posterior border closure of the mandible to a stable bilateral RCP. The clinician should try to achieve following objectives by removing these interferences,
- A maximum number of centric holding contacts are achieved in CR position.
- Vertical dimension in CR should be same or a little more than in CO position.
- Removal of interferences from CR to CO position, thereby facilitating smooth gliding movement in the horizontal plane from CR to CO.
The interferences are identified by placing blue marking tape between the teeth and asking the patient to “Squeeze” once the initial contact is made. Most commonly the mesial inclines of the maxillary lingual cusps and their opposing tooth surfaces are typical sites for supra-contacts. The mesial inner incline of the lingual cusp of the maxillary first premolars is the most common initial supra-contact at the RCP.

Step 2:
The second step is to achieve stable centric contacts in CO position. The occlusal contacts in the CO position should be planned in such a way that maximum stability of occlusion in this position is achieved. The primary objectives of clinician during this step are,
- Achieving a cusp to fossa relationship wherever possible as compared to cusp to marginal relationship. The cusp should contact, preferably at the center of the fossae so that occlusal forces are directed along the long axis of the tooth. However, it should be remembered that in unworn teeth (young patients), the cusp tips do not reach the base of the fossa. In such situation, multiple contacts on the inclined planes are considered as stable centric holding contacts.
- There should be no cusp contacts with the inclined planes except for the lingual surfaces of the maxillary anterior teeth.
The patient is asked to tap the teeth together on both sides at the same time. This is CO position where the maxillary and mandibular teeth are in maximum contact. Now, the wax is placed ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Step 3:
The third step is to remove excessive contacts from incisal surfaces. The objectives of this step are,
- Making the incisors slightly out of contact or in light contact over the maximum number of teeth.
- Eliminating supra-contact and hence trauma from occlusion on anterior teeth.
The firmness of the occlusal contact can be detected by placing a Mylar occlusal strip between the maxillary and mandibular anterior teeth held with a hemostat. The strip should just ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Step 4:
Protrusive excursion refers to the path of the mandible as it moves anteriorly between the CO and the edge to edge relationship of the anterior teeth (Figure 34.8). In this step, adjustment in protrusive excursions is done. The primary objectives of the dentist during this step are,
- Even distribution of contacts during protrusive excursions over as many teeth as possible. During the protrusive excursion, there should be no contact between the posterior teeth, except between the mesial slope of the buccal cusp of mandibular first premolar and the distal slope of maxillary cuspid.
- Reduction of the incisal edges of the extruded anterior teeth if they are interfering with the smooth protrusive excursion.
- Elimination of deep overbite by reduction of crown length of the anterior teeth. However, it must be remembered that it does not eliminate the requirement of orthodontic treatment. Only slight overbite can be eliminated by selective grinding. Moderate to severe cases require orthodontic treatment for deep bite correction.
The patient is asked to protrude the mandible slowly from CO position to edge to edge position of anterior teeth. Ideally, there should be bilateral contacts between maxillary and mandibular anterior teeth during this movement with little or no deviation of the mandible. The deviation usually is caused by a ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..

However, it should be preferred that wherever possible the adjustment is confined to the maxillary teeth to protect mandibular functional cusp height. Mandibular incisors should be ground only when the limit of grinding of the maxillary teeth has been reached because of pain, proximity to the pulp, or esthetic reasons. Following selective grinding, all the marks are removed and the patient is again asked to perform the protrusive movement. If posterior teeth are interfering with the protrusive movement, tooth structure is removed from the offending cusps until all articulating contacts between the posterior teeth have been eliminated.
Step 5:
This step deals with the removal or lessening of all interferences in lateral excursions. The mediotrusive interferences usually manifest as oblique facets on the first and second molar teeth on the inner inclines of the mandibular buccal cusps and the inner inclines of maxillary lingual cusps. The objectives of the dentist while eliminating lateral interferences are,
- A slight cuspid mediated disocclusion of the posterior teeth during the lateral excursion except in situations where cuspid is already worn and group function occlusion is present or cuspid is malposed and adjustment to group function of posterior teeth is necessary.
- Elimination of interferences on working side and balancing side.
- Elimination of interferences on central and lateral incisors which hinder the cuspid function during the lateral excursion except when both central and lateral incisors are in group function with cuspid and show no sign of trauma from occlusion.
While registering the lateral interferences, both habitual and passive (border) manipulation of the mandible is employed. A two-color method is used here in which the centric contact in CO are registered as blue and lateral supra-contacts are recorded in red color. For registering interferences on the working side, red ribbon is placed between the teeth in quadrant under question. Now, hold the mandible in CR position and ask the patient to close with moderate pressure. The patient is now asked to slide the mandible towards the right or left side, depending upon the side that has to be checked for working interferences. The red marks show interferences on the working side. Now, place a blue ribbon and without disturbing the red marks, establish the centric holding marks in CO position. To remove interferences, only undesirable red marks are removed. The inner inclines of maxillary buccal cusps or lingual surfaces of the upper anterior teeth are adjusted.

For registering interferences on the balancing side, a strip of adhesive occlusal registration wax is placed over the mandibular quadrant in question and another strip of folded occlusal registration wax is given to the patient that is placed on the opposite side and the patient is asked to chew this wax bolus up to five times. If there are ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
It should be remembered that while adjusting interferences on lateral excursion, reshape the inner inclines of the maxillary buccal cusps and mandibular lingual cusps. This is because grinding of the mandibular buccal cusps jeopardizes the functional cusps in CO position. Grinding should not result in the formation of flat surfaces and vertical stops should be preserved during the procedure.
Step 6:
This step deals with the elimination of undesirable gross occlusal features. Once all the interferences have been removed, there may be some remaining gross undesirable occlusal features which are harmful to the periodontal structures, and require modification. These include,
Extruded teeth:
These teeth are reduced to the level of the occlusal plane by grinding and reshaping within the limits permitted by proximity to the pulp.
Plunger cusps:
Plunger cusps are responsible for wedging of food in the interdental areas. Distolingual cusps of maxillary molars often are plunger cusps. These cusps should be rounded off and reshaped to eliminate food impaction.
Uneven adjacent marginal ridges:
These may also cause food impaction and should be corrected by either reducing the height of a comparatively high marginal ridge or increasing the height of a lower one with a restoration.
Rotated malposed and tilted teeth:
The most preferred treatment for rotated teeth is orthodontic de-rotation. However, minor rotations which interfere with the functional movement of the mandible or are causing food accumulation and impaction can be re-shaped by selective grinding.
Facets:
The wear facets are the result of the tooth to tooth wear. These can be easily detected by drying the tooth surface and viewing under a regular dental chair lamp. These should be corrected because the periphery of these facets may produce lateral or tipping forces which are deleterious to the periodontium.
Flat occlusal wear:
Sometimes excessive wear of the occlusal surfaces of the posterior teeth results in the formation of the flat occlusal surface. Similar to facets, the margins of the occlusal wear creates force component which causes lateral and tipping forces deleterious to the periodontium. The anatomy of the occlusal surfaces should be restored by selective grinding.
Step 7:
All the occlusal adjustments done are re-investigated in this step. All possible movements are done to check retrusive, protrusive and lateralotrusive interferences. In cases where occlusal equilibration can be better achieved by prosthodontic, restorative or orthodontic treatment, these treatments should be considered.
Step 8:
All the surfaces which have been selectively reduced are then polished to achieve smooth tooth surfaces and patient is instructed regarding the maintenance of teeth.
Correction of occlusal discrepancies prior to restorative procedures
Prior to restorative treatment, the present status of patient’s functional occlusion should be carefully evaluated. The occlusal corrections, if required, should be done prior to the restorative treatment. Dentition that requires multiple occlusal restorations either immediately or in future should be corrected for occlusal abnormalities. Following types of discrepancies are commonly observed and should be corrected prior to restorative treatment,
Marginal ridge discrepancies:
Marginal ridges of the posterior teeth that do not direct the food into the fossae promote food impaction in the inter-proximal region. Before restoring these teeth, opposing marginal ridge should be ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Extruded teeth:
Tooth extrusion is observed in the case where there is a massive coronal breakdown of the opposing tooth, or more frequently, if the opposite arch is edentulous. The extruded tooth should be corrected in conjunction with the restoration of the carious tooth or rehabilitation of the edentulous areas. It can be done by grinding or reshaping if the extrusion is slight or by installing a crown if the extrusion is excessive. If the extrusion is allowed to remain, it may result in functional disorders caused by occlusal interferences. Orthodontic treatment may be done to intrude the extruded tooth if extrusion is minor. However, it is difficult to intrude molars where extrusion is commonly seen. Sometimes, extrusion is so severe that intentional endodontic treatment of the extruded tooth followed by crown placement is required.
Plunger cusps:
Plunger centric holding cusps commonly result because of tipping and extrusion into a grossly carious opposing occlusal surface. The correction of the plunger cusps must be done prior to the restoration of the carious tooth. Simply reducing the height of the plunging cusp would be insufficient and would result in an excessively flattened cusp. The centric holding areas should be ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book ……. Contents available in the book……..
Broad opposing wear facets:
Broad wear facets should be eliminated by reshaping to permit the establishment of minimal centric contact areas. However, while reshaping the surface, stable centric stops must be preserved.
Wide occlusal tables:
The wide occlusal tables are usually a symptom of excessive occlusal wear. They should be narrowed to achieve stable centric holding areas by reshaping the cusp tips.
Rotated teeth:
If possible, the rotated teeth should be treated by orthodontic treatment. Orthodontic de-rotation brings the tooth in a proper position. If orthodontic treatment is not possible, moderate reshaping of the rotated tooth may improve the occlusion.
Our primary aim of the restorative treatment is not only to restore the decayed tooth or to replace the missing tooth, but also to provide a harmonious occlusion to the patient which functions smoothly without causing any discomfort to the patient. The understanding of the basic principles of occlusion is essential to achieve this goal. It should be remembered that occlusal adjustments should be well planned because an improper treatment my worsen the existing problems of the patient.
Conclusion
A comprehensive TMJ and occlusal examination is an inseparable part of the complete periodontal examination. The neuromuscular harmony is the prime requirement for appropriate TMJ function and functional mandibular movements. However, it should be remembered that a thorough knowledge of occlusion is required to treat the condition otherwise the situation may worsen after the treatment. Therefore, clinical examination, which consists of the examination of the TMJ, teeth, soft tissue as well as the periodontium, should be carried out before the commencement of dental treatment. The occlusal examination and identification of the interferences should be done and in a stepwise manner, all the interferences should be eliminated.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.