Introduction to Lasers
Periodontal diseases consist of a group of inflammatory diseases initiated by bacteria that colonize the teeth and infect their surrounding soft tissues. Bacteria and their products contaminate the root surface and make it biologically incompatible for soft tissue attachment. It is well established that a clean root surface is mandatory for the stability of the fragile attachment between the root surface and the gingival flap by the maturing fibrin clot 1. Scaling and root planning are the traditional methods of controlling subgingival microflora for the management of periodontal diseases. The objectives of subgingival debridement are to eliminate not only the adherent and unattached bacterial plaque, but also deposits of calculus. Scalers and curettes have been used traditionally to achieve a clean and smooth root surface which is biologically compatible for soft tissue attachment. Lasers are the most recent introduction in the treatment of periodontal diseases. Presently, they are used for the removal of calculus and root surface detoxification, removal of the lining epithelium of the diseased pocket wall, and for their antimicrobial effect on the pocket microbiota.
The word LASER is an acronym for light amplification by stimulated emission of radiation. Lasers have been used extensively in the medical field since they were introduced. Soon after their introduction into the medical field, lasers for dental use were introduced. Presently, there are a wide variety of lasers available for dental use. In the following discussion, we shall read in detail about the use of lasers in periodontal treatment.
History of Lasers in dentistry
The first laser device was made by Maimanin in 1960 2, based on Albert Einstein’s theory of “spontaneous and stimulated emission of radiation” in the early 1900s. In 1961, Snitzer described the prototype for the Nd:YAG laser. In dentistry, first laser introduced was the ruby laser by Goldman in 1964 3. The next major advancement in the development of laser technology for soft tissue use was the introduction of a contact delivery system for the Nd: YAG laser in 1984 4. After that, many lasers such as …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Principles of working of a LASER
As already stated, the principles of laser action were first proposed by Albert Einstein in 1917. The functioning of LASER is based on the concepts of probability coefficients (termed ‘Einstein coefficients’) for the absorption, spontaneous emission, and stimulated emission of electromagnetic radiation. To understand the functioning of LASER, let us consider two energy levels (E1 and E2) of electrons, where, E1 is the ground state or lower energy state of electrons and E2 is the excited state or higher energy state of electrons. When a photon that has energy equivalent to the difference between the two energy levels (E2 – E1) is incident on the atom, the electrons jump from the ground state (E1) to the excited state (E2). It must be noted here that absorption of radiation or light occurs only if the energy of the incident photon exactly matches the energy difference of the two energy levels …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..

In spontaneous emission, the electron moves from the higher energy state to the lower energy state naturally, thus, we have no control over when an excited electron is going to lose energy in the form of light. Furthermore, photons emitted in the spontaneous emission process constitute ordinary incoherent light, that is, the photons emitted in the spontaneous emission process do not flow exactly in the same direction of incident photons. That is why a stimulates emission is required to generate a LASER beam. In stimulated emission, the incident photon forces the excited electron to return to the ground state. Here, energy in the form of a photon is supplied to the excited electron instead of supplying light energy to the ground state electron. In stimulated emission, two photons are emitted. One photon is due to the incident photon and another one is due to the energy release of excited electron. The process of stimulated emission is very fast as compared to spontaneous emission. The photons emitted during stimulated emission have the same …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Fundamentals of Lasers
As already stated, the word LASER stands for light amplification by stimulated emission of radiation. Let us first try to understand the five words used to describe laser.
Light:
Light is a form of energy manifesting itself as electromagnetic radiation and is closely related to other forms of electromagnetic radiations such as radio waves, radar, microwaves, infrared and ultraviolet radiations, and X-rays. The basic unit of this radiant energy is called a photon. Light can be defined by two basic properties: amplitude and wavelength. Amplitude is defined as the vertical height of the wave oscillation from the zero axis to its peak. Wavelength is the horizontal distance between any two corresponding points on the wave. Frequency is a measurement of how many cycles can happen in a certain amount of times (cycles per second). Frequency is inversely proportional to wavelength: the shorter the wavelength, the higher the frequency, and vice versa. These properties of light waves are very important because they determine the energy of the laser beam and its effect on the soft and hard tissues.

Amplification by stimulated emission:
To understand how amplification by stimulated emission occurs, we should know the components of laser instrument. A laser unit is made up of an optical cavity, the core of which is made up of chemical elements, molecules, or compounds called the active medium. An excitation source surrounds the core of the optical cavity which may be a flash lamp strobe device, an electrical circuit, or an electrical coil. This excitation source pumps the energy into the active medium. On the two ends of the optical cavity, two mirrors are placed parallel to each other. In the case where semiconductors are used as the active medium, polished surfaces replace the mirrors. The mirrors act as resonators and help to collimate and amplify the developing beam. Other components of the laser unit are a cooling system, focusing lenses and some other controls.
To understand stimulated emission we must also know the basics of quantum physics. Max Planck and Neils Bohr described the quantum theory of physics according to which a quantum is the smallest unit of energy emitted from an atom. Later on, Einstein further theorized this concept and stated that an additional quantum of energy …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Radiation:
Radiation is a form of electromagnetic energy. The electromagnetic spectrum is composed of a wide spectrum of waves which have different wavelengths and energies. The smallest wavelength is that of gamma rays (10-12 meters) and largest wavelength is for radio waves ranging upto thousands of meters. Figure 57.2 describes various electromagnetic waves in the electromagnetic spectrum.
Characteristics of laser light
The laser light is collimated (parallel) and coherent (temporally and spatially constant) electromagnetic radiation of a single wavelength. Laser light is monochromatic because it only generates a laser beam of a single color, which is sometimes invisible. Laser light is produced by pumping (energizing) a certain substance, or gain medium, within a resonating chamber. The laser light is produced when an excited atom is stimulated to emit a photon. The spontaneous emission of a photon by one atom stimulates the release of a subsequent photon and so on. In this way, a very coherent and synchronous wave, of a single wavelength in a collimated form is produced.
There are two basic modes of wavelength emission for dental lasers, based on the excitation source: continuous wave emission and pulsed emission. In continuous wave emission, the laser energy is emitted continuously as long as the laser is activated (example CO2 laser). The pulsed emission may be delivered in two different modalities: a free-running pulse, in which …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Classification of lasers
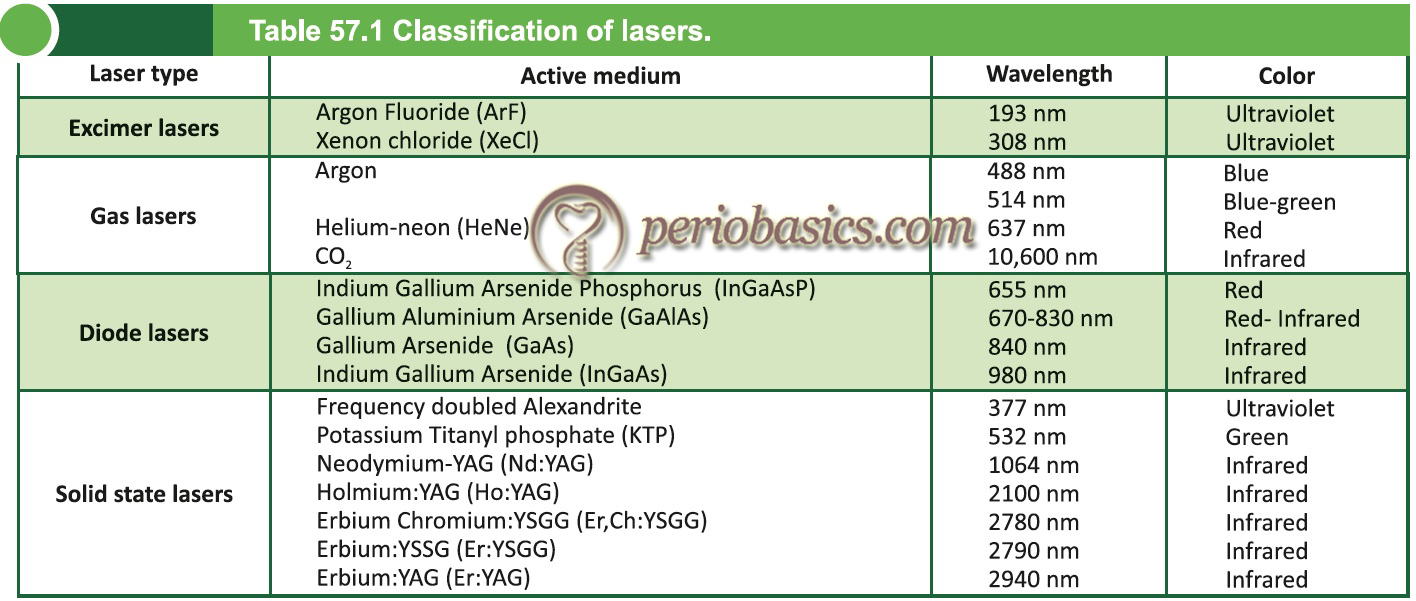
The lasers can be classified on the basis of the type of active medium and characteristics of the laser light. On the basis of active medium or gain medium, they are classified into four classes: Excimer lasers, Gas lasers, Diode lasers and Solid-state lasers. On the basis of the characteristics of the laser light, they can be classified as soft and hard lasers. Soft laser irradiation takes place at thermal, low-energy settings at wavelengths believed to stimulate circulation and cellular activity. Hard lasers (through thermic or ablative effects) have been used extensively for surgical applications 5, 6.
Effect of lasers on soft and hard tissue
There are four things which may happen when the laser light strikes the tissue:
Reflection.
Transmission.
Scattering.
Absorption.
Reflection occurs when the laser beam is simply redirected off the tissue surface, exerting no effect. When used on the tissue, the minimum amount of laser radiations is reflected from the surface. Second is the transmission, which refers to the passage of laser through the tissue without exerting any effect on the target tissues. Transmission of laser light depends on the composition of tissue. For example, water is relatively transparent to the diode and Nd:YAG wavelengths. On the other hand, Erbium and Carbon dioxide laser beams are readily absorbed by tissue fluid and a very little energy is transmitted to the adjacent tissues. Scattering is the dispersion of the laser beam into low energy radiations which have …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
The fourth effect is absorption, which refers to the absorption of the laser beam energy by intended target tissue, resulting in its usual desirable effect. Absorption of the laser beam depends on various factors such as the wavelength of the laser beam, water content of the tissue, pigmentation, and emission mode. The absorption coefficient strongly depends on the wavelength of the incoming laser irradiation. Neodymium : yttrium aluminum garnet (Nd:YAG) and diode lasers are preferentially absorbed by pigmented tissues. The CO2 laser is well suited for soft tissue surgery, as its energy is highly absorbed by water. Other parameters which affect the absorption of the laser radiation are power, pulse duration, duration of exposure, angle of energy delivery and waveform (i.e., pulsed or continuous).
When lasers are used, they can be used in contact mode or non-contact …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Biologically, five types of effects can be seen when the laser beam photons enter a tissue. These are,
1. Fluorescence.
2. Photothermal effect.
3. Photodisruptive effect.
4. Photochemical reaction.
5. Photobiomodulation.
Let us now discuss these effects of laser radiation on tissues in detail.
Fluorescence:
Fluorescence is the property of an object of absorbing light of short wavelength and emitting light of longer wavelength. In laser application on the tooth structure, fluorescence occurs when the carious lesion is exposed to the 655 nm visible wavelength. It helps in the diagnosis of early carious lesions.
Photothermal effects:
When the energy of the laser beam is converted into heat, it is referred to as a photothermal effect. This heat produced is used to perform functions such as incising tissue or coagulating blood. The heat produced by the laser beam has variable effects on tissues which depend on the energy of the laser beam. When a laser heats oral tissues, certain reversible or irreversible changes can occur:
Hyperthermia: below 50⁰C.
Coagulation and protein denaturation: >60⁰C.
Vaporization: >100⁰C.
Carbonization: >200⁰C.
Irreversible effects such as denaturation and carbonization result in thermal damage that causes inflammation, pain, and edema in the tissue.
Photodisruptive effect:
Photodisruptive or photoacoustic effect results when the laser beam with extremely high power interacts with water, causing rapid thermal expansion of the water molecules. It results in a thermo-mechanical acoustic shock wave that is capable of disrupting enamel and bony matrices, quite efficiently. The micro-explosions which are created in the hard tissue matrix lead to its disruption and thus creating micro-fractures. This shock wave creates the distinct popping sound heard during erbium laser use.
Photochemical reaction:
Photochemical reactions occur when the photon energy causes a chemical reaction. These reactions are implicated in some of the beneficial effects found in biostimulation.
Photobiomodulation:
Photobiomodulation or biostimulation refers to the modulatory effect of laser radiation on cellular response. Many studies have exhibited effects such as increased collagen synthesis, fibroblast proliferation, increased osteogenesis and enhanced leukocyte phagocytosis with various wavelengths of laser. The exact mechanism by which the laser radiation …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Various lasers available for periodontal use
Lasers have been used for various periodontal treatments. The most common lasers used for periodontal treatments are carbon dioxide (CO2), neodymium:yttrium-aluminum-garnet (Nd:YAG) and erbium:yttrium-aluminum-garnet (Er:YAG) and diode lasers. Let us now discuss these lasers in detail,
Carbon dioxide (CO2) laser
The CO2 laser has a wavelength of 10,600 nm and can be used in either pulsed-wave or continuous-wave modes. Its absorption coefficient in hydroxyapatite is very high (104), but the absorption coefficient in water is low (103), accounting for the powerful ablative properties of this laser 11. The CO2 laser beam is absorbed in the tissue surface with very little scatter or penetration. Therefore, this laser is very effective for soft tissue surgeries. It produces severe thermal damage, such as cracking, melting, and carbonization when applied to hard tissues 12, 13. The major advantage of a CO2 laser is its strong hemostatic and bactericidal effect. It was approved by the Food and Drug Administration (FDA) 1976 for soft tissue surgeries.

Various studies have been done to evaluate the effect of CO2 laser on calculus-afflicted root surfaces. In one scanning electron microscope (SEM) study, morphological changes on the root surface were evaluated following CO2 laser application. Observations showed that laser application induced charring, meltdown, and re-crystallization of calculus minerals. The authors advocated the adjunctive use of CO2 laser with traditional methods of calculus removal 14.
It has been shown that excessive removal of cementum and dentin after CO2 laser application may result in dentinal hypersensitivity and cervical de-mineralization 15. This phenomenon has been explained on the basis of waveguide theory, according to which, when laser energy is redistributed along the interface of two dissimilar layers, the bond between these layers is weakened. This may happen at cemento-dentinal junction resulting in excessive cementum removal during laser scaling 16.
The effectiveness of CO2 laser has also been evaluated for smear layer removal from the root surface. In one study, the effectiveness of smear layer removal by …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Neodymium-doped: Yittrium-Aluminium-Garnet (Nd:YAG) laser
This is a solid-state laser having a slightly longer wavelength (1,064 nm) than diode lasers. This wavelength has low absorption in water and is absorbed by pigment in the tissue. This laser is very effective in producing hemostasis and coagulation in soft tissue. Thus, Nd:YAG laser is mainly used for ablation of potentially hemorrhagic soft tissue. The width of coagulation ranges from 0.3 to 0.8 mm at 3-10 W of laser power.
Nd:YAG laser has been studied for its effect on root surface also 18-21. It has been shown that Nd:YAG laser usage on root surface may result in the crater formation, charring, and surface contamination …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..

One study examined the effect of Nd:YAG lasers on endotoxin in teeth extracted due to periodontal disease. It was found that the laser alone could not produce a high enough temperature to destroy cementum-bound endotoxins and still remained within safe clinical limits. Scaling and root planing (SRP) alone or combined with laser treatment produced similar outcomes in terms of the reduction of IL-1β for up to 3 months 22. Many authors have suggested that Nd:YAG laser should be used as an adjunct to SRP to perform sulcular debridement rather than to remove calculus 23, 24. This is because attachment gain has been observed after its application for pocket debridement, which is mainly due to the elimination of bacteria from the periodontal pocket. As the pocket epithelium in a diseased environment consists of significant granulation tissue (which is dark-colored due to dilated blood vessels), the laser could stimulate evaporation of the darker tissue thus reducing periodontal pathogens and prolonging their recolonization time 25. While using the laser tip subgingivally, its tip should only be brushed over the periodontal pocket surface for a sufficient duration of time.
In a study which compared SRP alone and SRP+ Nd:YAG laser application, it was found that the pocket depth reduction was 1.6 mm and 1.7 mm for SRP and SRP+ Nd:YAG laser …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Erbium : Yttrium-Aluminium-Garnet (Er:YAG) laser
This laser has a wavelength of 2,940 nm (2.94 µm), and very high absorption coefficients in water and hydroxyapatite compared to the diode and Nd:YAG lasers. It has been widely studied for its effect on pocket debridement. This laser works through the generation of “shock waves” in the tissue because of its high absorption in water molecules. As the very high energy laser beam is absorbed by water molecules, micro-explosions are produced creating these shock waves.
When applied on hard tissue like tooth structure, it produces micro-fractures due to this phenomenon. It was the first dental laser to receive approval for the preparation of dental cavities 27. As for other lasers, its effect on root surface has been extensively investigated. Erbium lasers show the greatest potential for effective root debridement. The Er:YAG laser has been shown, in vitro, to remove calculus 28 and to negate endotoxin 28-31. However, application of Er:YAG laser has also been shown to damage the root surface. Studies have shown various effects of Er:YAG laser treatment on cementum surfaces of extracted teeth, including cratering and heat cracking, regardless of the presence of water coolant 32, 33.

This laser has bactericidal effects. Its bactericidal effects were observed against P. gingivalis and A. actinomycetemcomitans even at low energy level 34. The factor that contributes to its bactericidal activity is that the wavelength of Er:YAG laser corresponds to the peak of absorbance of bacterial lipopolysaccharide, and hence the Er:YAG laser can effectively and rapidly remove most of the lipopolysaccharide that coats the teeth 35. Er:YAG laser has also been proposed for the implant maintenance, taking advantage of its bactericidal or decontamination effect. It has been shown that debridement of implant abutment surface by Er:YAG laser resulted in the effective removal of plaque and calculus without producing damage to the implant surface 36. Another study observed a nonexcessive heat generation on the implant surfaces and effective decontamination by means of the Er:YAG laser 37.
Clinically, when Er:YAG laser is used subgingivally with a water coolant, it causes a splash of water and blood from pockets as the result of explosive ablation and so it requires an extraoral …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Diode lasers
These lasers are made up of solid-state semiconductors with wavelengths in the infrared region of the electromagnetic spectrum. Most commonly used diode lasers are …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Depending on the energy of the laser beam, two types of diode lasers have been studied: the high-level diode laser (which emits high intensity light energy), and the low-level diode laser (which emits low-intensity light energy). The diode lasers with high levels of energy are used for soft tissue surgery and for curettage. They also produce a very good hemostasis and are mainly used on soft tissues. Low-level diode lasers are used for biostimulation. The low energy laser application on soft tissue has been shown to modulate the cellular response thereby promoting healing.

In an in vitro study, Kreisler et al. (2003) 40 evaluated the proliferation rate of human periodontal ligament fibroblasts when irradiated with low-level diode laser. Human periodontal ligament fibroblasts were cultured and irradiated with an 809 nm wavelength diode laser. The rate of proliferation, determined by relative fluorescence units, was checked at 24, 48, and 72 hours after irradiation. The results indicated that cells in the test group (irradiated) demonstrated a considerably higher proliferation activity than the controls. The differences were discernible up to a 72-hour observation time, and those differences were statistically significant. The same authors suggested that the laser treatment may be beneficial in regenerative periodontal therapy.
Bactericidal action of diode lasers has also been demonstrated in various investigations. In one study a diode laser at 810 nm wavelength was used in a rat model to evaluate its effect on bacteria in periodontal pockets. In this study, bacterial samples were taken from periodontal pockets before and after subgingival laser irradiation. The microbiological analysis showed that bacteria such as Prevotella spp., β-hemolytic Streptococci, Fusobacterium spp., and Pseudomonas spp. were significantly reduced, following the laser application 41.
Diode lasers also demonstrate anti-inflammatory action on the tissue. As we know that bacteria and their products induce an inflammatory response which is mediated by the release of a variety of mediators. Prostaglandins (PGE2) and cyclooxygenases (COX) are one of these mediators which have been involved in bone resorption in periodontal and endodontic lesions. In one study, Sakurai et al. (2000) 42 challenged human gingival fibroblasts with lipopolysaccharides of bacterial origin. After irradiation with a diode laser, the amount of PGE2 was detected by radioimmunoassay, and levels of mRNA were detected. The results indicated that the irradiated cells did produce considerably less PGE2 and COX, indicating the possible anti-inflammatory role of the diode laser, thus modulating the host response.
In one in vivo study on 50 patients, Moritz et al. (1998) 43 studied the effect of subgingival irrigation with H2O2 and 810 nm diode laser on the subgingival microbiota. Patients were randomly subdivided into two groups. Subgingival bacteria samples were collected in all patients. Patients were treated either with laser or subgingival irrigations of H2O2. After 6 months, the final values of the periodontal indices and further microbiological samples were measured. The total bacterial count, as well as specific bacteria (e.g., A. actinomycetemcomitans, P. intermedia, and P. gingivalis), were assessed …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Clinical technique for laser treatment
A variety of laser units for periodontal therapy are available commercially, these days. Although, every laser unit is provided with usage instructions, following is the description of general guidelines followed during laser treatment.
- Usually, topical anesthesia is adequate, but if required local anesthesia is administered in the area to be treated.
- The operator, the patient, and the assistant must wear the protective eye glasses to prevent accidental damage by the laser beam.
- Laser units come with various power settings for various treatments such as inner epithelium lining removal, outer epithelium removal or calculus removal. The required setting is selected for the treatment.
- For pocket lining removal, the tip of the laser is placed in contact with the gingival crest, parallel to the long axis of the tooth. The laser is activated and is moved along the gingival margin to prepare a trough all the way to the crest of the bone. The radial and forward cutting action of this tip allows for effective separation and simultaneous removal of the inflamed and diseased epithelial lining. The narrow tip glides easily to allow minimally invasive treatment of the entire epithelium lining all the way to the bottom of the pocket. Alternatively, the bottom-up technique can also be used, activating the laser at the bottom of the pocket, moving it coronally.
- For outer gingival epithelium removal, the tip of the laser is kept parallel to and approximately 1 mm away from the outer gingiva. Angle the end of the tip slightly toward the surface. The activated laser tip is moved over a 5 mm area from the gingival margin apically. The tissue surface is altered only enough to disrupt the epithelial layer, without significant tissue removal.
- For calculus removal, hand or ultrasonic scaler may be used prior to laser application. Calculus removal is performed with the fiber tip at 10-15 degree angle against the surface moving up and down in one pass followed by a side-by-side pass. The root surface is checked after every motion with the help of loupes for the presence of remaining calculus. After removal of the calculus, root surface smoothening settings are used to refine the root surface.
- Following any of the above procedures, a curette is inserted into the pocket to push the gingiva away and visualize the root surface. The surface should be clean and free of any calculus deposits. External pressure should be applied with the help of a wet gauge for approximately 3 minutes to produce a thin layer of blood clot inside the pocket. The clot within the sulcus is sealed by applying a barrier such as surgical glue (cyanoacrylate).
- The patient is instructed not to use a toothbrush for the first 24 hours after the procedure. After 24 hours, the patient is asked to start brushing again using a soft-bristle toothbrush and toothpaste, floss daily, and use an over-the-counter mouthwash rinse after 2-weeks. The patient is scheduled for follow-up visits, including the first probing at 3 months.
Applications of lasers in periodontal therapy
Lasers have been widely used in periodontal treatment. They have been investigated for their use in promoting periodontal attachment 44, elimination of bacteria from periodontal pockets 34, debridement of root surfaces 45 and treatment of dentinal hypersensitivity 46.
Debridement of the root surfaces:
Prime requirement for a laser to be used for the debridement of root surfaces is the effective removal of calculus from the root surface without causing any thermal damage to the pulp tissue and unwanted removal of the sound root structure. This can be achieved only by the use of wavelength with minimal penetration depth in mineralized tissue. Various lasers used for this purpose include CO2, Nd:YAG, Er:YAG, and diode lasers. Until 1994, CO2 and Nd:YAG lasers were used for calculus removal from root surface, but it was seen that the calculus removal was either incomplete or fraught with potential damage to the surrounding tissues 14, 47, 48.
With the introduction of Er:YAG and Er,Cr:YSGG lasers and frequency-doubled alexandrite (FDA, 377 nm), the calculus removal from the root surface was improved with less damage to the root surface …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Various studies have been done to evaluate root surface cleaning efficacy of various lasers. One study demonstrated efficient calculus removal with no side effects and uneventful reduction of pocket depth after Er:YAG scaling 49. Another study reported that equal or slightly better results were observed at six months after laser treatment of periodontal pockets as compared to conventional mechanical debridement using hand scalers and found a significantly higher reduction in bleeding on probing scores and improvements in clinical attachment 46.
However, laser application on root surface has also been shown to cause root surface damage. The power of the laser beam, duration of application and the technique of application are various factors which determine the effectiveness of lasers in root surface debridement without causing collateral damage.
Removal of the diseased pocket epithelium:
Almost all the laser wavelengths have been investigated for their efficacy in pocket epithelium elimination. Added to the current wavelengths is the recent development of a frequency-doubled (wavelength-halved) Nd:YAG laser at 532 nm, termed, the KTP laser, which has a range of action similar to that of the 810 nm diode laser. ‘KTP’ denotes potassium titanyl phosphate, which is the crystal used to affect the frequency doubling of the 1,064 nm wavelength 50. Lasers have …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Hemostasis:
One of the primary advantages of laser therapy over conventional scalpel surgery is its superior hemostasis. Along with precise incision and excision, hemostasis is one of the many results of the photothermal events that take place when the laser is applied to the soft tissue. CO2 laser has a very good hemostatic capability. Gingivectomy for gingival overgrowth is a typical indication for CO2 laser treatment. Nd:YAG laser is also very effective at producing coagulation and hemostasis, in a relatively thick layer of soft tissues. It is very effectively used for ablation of potentially hemorrhagic soft tissue, with the width of coagulation ranging from 0.3 to 0.8 mm at 3-10 W of laser power. Diode lasers are also very effective in achieving hemostasis.
Bactericidal effects:
The eradication of subgingival microbiota and bacterial endotoxins from the root surfaces is an important factor in the outcome of periodontal therapy. Research has shown that lasers are effective in bacterial elimination, resulting in a better healing. In periodontally involved teeth, deep bacterial invasion of the radicular dentin has been demonstrated 53. The bacteria in the dentinal tubules can serve as a reservoir for the re-colonization of the instrumented root surface. It has been shown …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..
Frenectomy:
Lasers have been used for frenectomy procedure. Studies have shown the superiority of laser over the conventional scalpel method which includes hemostasis effect, excellent visualization of the operating field, reduced operating time, less need for local anesthesia, sterilization of the wound site; elimination of suturing, reduction of postoperative edema and pain and minimal scarring 56-61. CO2, Er:YAG, Nd:YAG, Er,Cr:YSGG, diode, and diode in conjunction with Er:YAG lasers …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book …….. Contents available in the book ……..



De-pigmentation:
Hyperpigmentation of gingiva occurs due to the deposition of melanin in the basal and suprabasal layer of the epithelium, creating an un-esthetic appearance. Various procedures used for the elimination of pigmentation include scalpel surgery; gingivectomy with free-gingival autografts or allografts, electrosurgery and cryosurgery, abrasion with diamond burs and lasers. Presently, laser is commonly used for the de-pigmentation. The main advantages associated with laser-assisted de-pigmentation are short treatment time and hemostasis.


Advantages and disadvantages of lasers in periodontal therapy
Advantages of lasers in periodontal therapy:
- Effective and efficient soft and hard tissue ablation with a greater hemostasis, bactericidal effect, minimal wound contraction, minimal collateral damages with reduced use of local anesthesia.
- Lasers are most useful for the removal of hemorrhagic lesions.
- Bloodless operative field, thus better visibility.
- They have a high patient acceptance.
- Many procedures can be done with only topical anesthesia.
- Better healing and less scarring.
- Less time-consuming.
- The hard‐tissue laser devices can selectively remove the diseased tooth structure because a carious lesion has a much higher water content than healthy tissue, and water is the primary absorber of that wavelength of laser energy.
Disadvantages of lasers in periodontal therapy:
- Laser light interacts with target tissues not only in the contact irradiation mode but also in the non-contact irradiation mode. Therefore, use of glasses for eye protection ( by the patient, operator, and assistants) is required.
- The laser beam may be reflected off shiny metal surfaces of dental instruments, such as retractors or mouth mirrors, which can cause accidental irradiation to the adjacent tissues. Wet gauze packs may be occasionally useful for protection of the oral tissues surrounding the surgical site from accidental beam impact 65.
- High-speed evacuation is necessary to capture the laser plume, which is a biohazard 66.
- Er:YAG and CO2 lasers may cause melting or ablation of tooth structure if they come in contact with tooth structure.
- The cost of laser apparatus is high.
Conclusion
The conventional non-surgical and surgical periodontal therapy is the primary line of treatment of periodontal diseases. However, complete access and disinfection of periodontal defects may not be achieved by mechanical instruments. Furthermore, the bacterial invasion cannot be eradicated by mechanical debridement alone. The application of laser facilitates the disinfection of the difficult to reach diseased root surfaces and elimination of periodontopathic bacteria. In the above discussion, various lasers have been discussed with their properties and clinical applications. It can be concluded from the above discussion that laser is an useful adjunct to the conventional periodontal therapy. In future, many advancements in both soft and hard tissue lasers are expected.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.