Introduction to gingivitis
It has been well established that diseases are initiated by oral bacteria perturbing epithelial cells, which trigger innate, inflammatory, and adaptive immune responses. These processes result in the destruction of the tissues surrounding and supporting the teeth and eventually result in tissue, bone, and, finally, tooth loss. Lipopolysaccharide (LPS) is a cell wall constituent of virtually all subgingival Gram-negative microorganisms 1. These molecules are known to induce PMN leukocyte infiltration in the inflamed periodontal tissues, edema, vascular dilatation, stimulation of osteoclasts, and collagen phagocytosis 2-5. LPS is a potent inducer of inflammatory cytokine synthesis (IL-1, PGE2, TNFα, IL-6 and IL-8) 6-8. The available data suggest that periodontal diseases are multi-factorial diseases. There are several factors that amplify the inflammatory process, making some individuals more susceptible to periodontal disease than others. Patient susceptibility is one of the most important factors that determine the outcome of periodontal diseases. While periodontal bacteria are the primary etiological agents, the host immune response to these bacteria is of fundamental importance 9. In the following discussion, we shall discuss the development of gingivitis, its immunological aspect, and its clinical features in detail.
Classification of gingivitis
According to duration:
- Acute gingivitis: It is of sudden onset and short duration and can be painful.
- Chronic gingivitis: It is slow in onset and is of long duration. It is painless unless complicated by acute or subacute exacerbation. It is the most common type of gingivitis.
According to distribution:
Localized gingivitis: (Confined to the gingiva of single tooth or a group of teeth)
- Localized marginal gingivitis (confined to one or more areas of the marginal gingiva).
- Localized diffuse gingivitis (extends from the margin to the mucobuccal fold but in a limited area).
- Localized papillary gingivitis (confined to one or more interdental spaces in a limited area).
Generalized gingivitis: (Involves the entire mouth)
- Generalized marginal gingivitis (involves the gingival margins in relation to all the teeth).
- Generalized diffuse gingivitis (involves the entire gingiva.).
Historical aspect
The development of gingivitis has been extensively studied in animal 10 and human models 11, 12, 14. In 1976, Page and Schroeder 10 published the classical histological studies on the progressive “natural history” of experimental periodontal disease lesions in dogs. The dogs which were first given meticulous oral hygiene, were subsequently placed on soft foods (non-cleansing) and deprived of any oral hygiene. Their work described four types of lesions representative of stages of disease:
Initial lesion:
The initial lesion begins within 2-4 days after deprivation of oral hygiene. In this stage, we can see a few neutrophils in the junctional epithelium, which are in the process of migration into the gingival crevice. There are small numbers of macrophages and lymphocytes in the connective tissue, and the lymphocytes are primarily T-cells. The distribution of cell types within the periodontal arena is not uniform. As stated above the neutrophils infiltrate the junctional epithelium and gingival crevice, whereas, lymphocytes and other mononuclear cells are within the subjacent connective tissue 10, 13.
Main histological findings:
- Vascular dilation and vasculitis subsequent to the junctional epithelium.
- Infiltration of polymorphonuclear neutrophils (PMNs) into the junction and sulcular epithelium.
- Predominant immune cells are PMNs.
- Perivascular loss of collagen.
- Alteration of the coronal part of the junctional epithelium.
Early lesion:
It evolves from initial lesion within 4-7 days and continues up to 14 days. Histological examination shows a marked ………… Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book…….

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Established lesion:
After 14 days, the neutrophil infiltration of the pocket and the junctional epithelium is intense. B-cells undergo blast transformation and conversion to plasma cells (with local production of antibody) and monocytes derivatives clearly look like macrophages. Page and Schroeder suggested that the established lesion was extremely prevalent in man, and could be stable for many years.
Main histological findings:
- Vascular proliferation and blood stasis.
- More advanced area of rete-peg formation and atrophic areas in the sulcular and junctional epithelium.
- Predominant immune cells are plasma cells.
- Continued collagen loss.
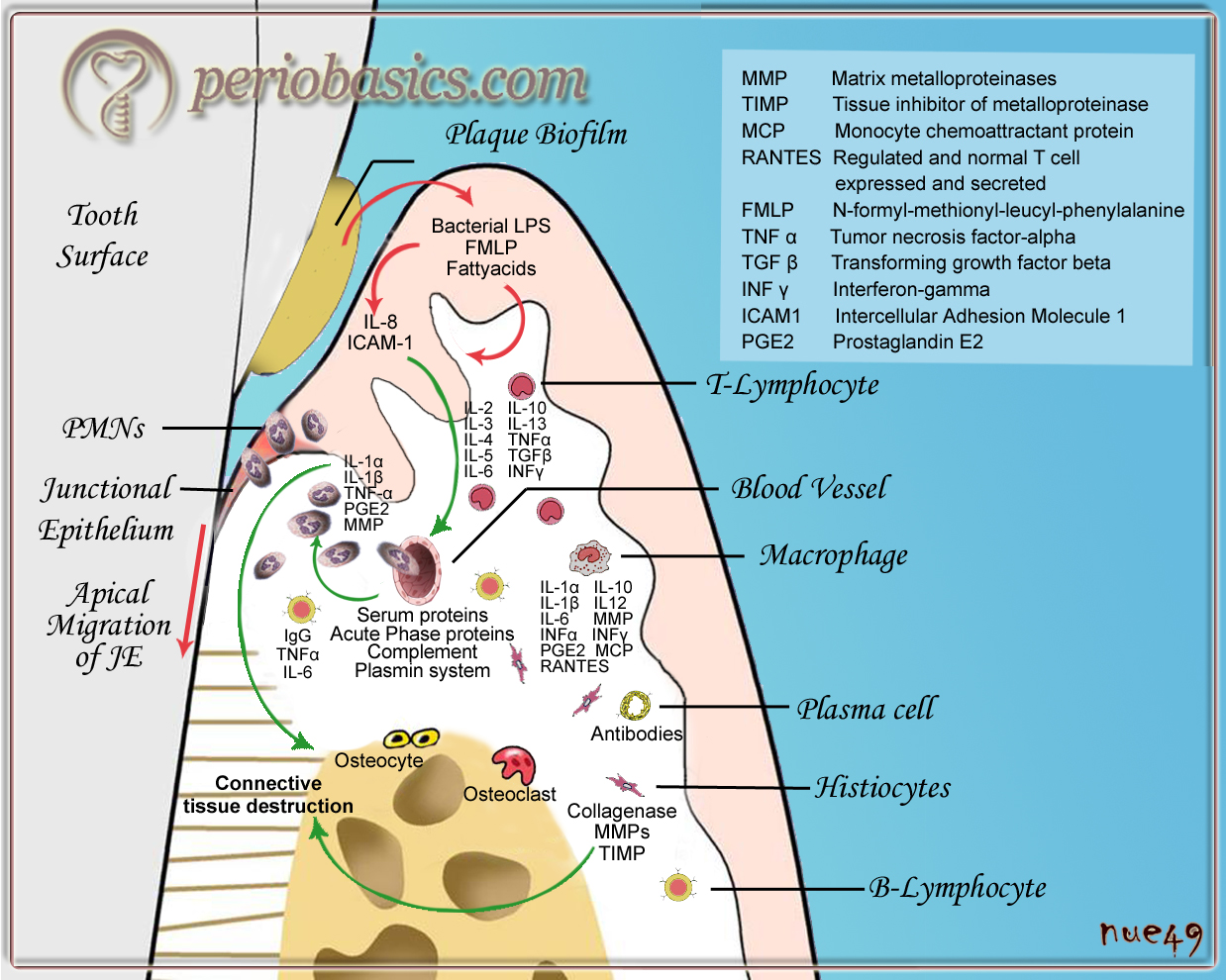
Advanced lesion:
The lesion is considered advanced when the destruction of bone is evident. At this late stage, the pocket epithelium shows ulceration, junctional epithelium shows great apical extension. Plasma cells continue to dominate the connective tissues, and neutrophils continue to dominate in the junctional epithelium and gingival crevice. Many of the plasma cells appear to be “degenerating” 10, probably normal apoptosis, in retrospect. One of the proposed mechanisms for the release of the cytokine, interleukin-1β (IL-1β), may involve apoptosis since IL-1β is activated by the cytosolic enzyme important in apoptosis (caspase-1; aka “interleukin-1β converting enzyme [ICE]”).
Main histological findings:
- Predominant cells are plasma cells.
- Further destruction of collagen subjacent to the junctional epithelium is seen, with fibrosis at distant sites.
- A prime characteristic of the advanced lesion is the extension of the lesion into the periodontal ligament and supporting bone.
- Finally, there is bone loss that is exhibited as clinical attachment loss and pocket formation.
From above discussion, we can conclude that:
- All of these lesions except the advanced lesion represent what we would call “gingivitis,” from the clinical perspective.
- Neutrophils are the first leukocytes to arrive.
- In the pathogenesis of periodontal disease, neutrophils are always the dominant cell type within the junctional epithelium and gingival crevice.
- Periodontitis progresses from gingivitis and this transition occurs after B-cell activation to the plasma cell.
Our current understanding of the periodontal immune response
Presently, we have overwhelming evidence that periodontal pathogens and their products, as well as inflammatory mediators produced in periodontal tissues, are responsible for periodontal connective tissue degradation. Let us try to understand how the host immune response is generated against microbial insult and the initial lesion progresses to form an established lesion.
Early reaction to plaque accumulation:
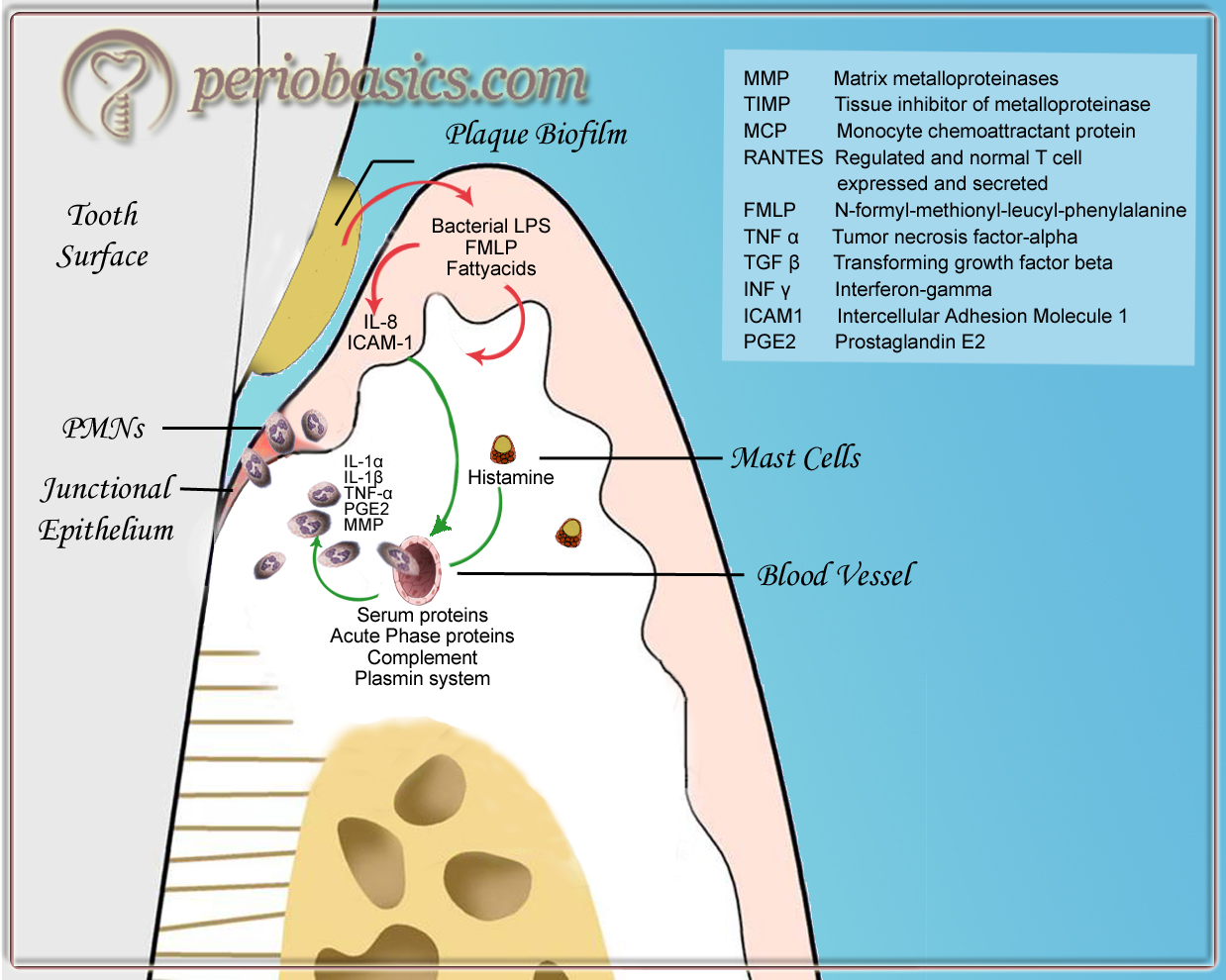
- The bacteria present in the plaque produce various substances which can initiate vascular events of acute inflammation. These products are metabolic acids, bacterial lipopolysaccharides, FMLP (N-Formyl-Methionyl-Leucyl-phenylalanine), volatile sulfur compounds, extracellular enzymes and fatty acids.
- These mediators stimulate the cells of junctional epithelium to produce various inflammatory mediators like interleukin-8 (IL-8), tumor necrosis factor-α (TNF-α), prostaglandin E 2 (PGE2), interleukin-1α (IL-1α) and 2 matrix metalloproteinases (MMPs).
- Neuropeptides and histamine produced by free nerve endings cause vascular effects in that area. These mediators cause increased vascular permeability.
- Perivascular mast cells produce histamine, which causes the endothelium to release IL-8 which leads to the PMN recruitment.
- Because of the alteration in the vasculature in that area, plasmin which is a part of the fibrinolytic system, gets involved in the inflammatory response. It causes degradation of fibrin. Degradation products of fibrin further promote vascular permeability.
- All these events lead to the alteration in gingival vascular plexus. The vessels proliferate, and a distinct loop formation occurs in the small vessels directly below the basement membrane of the sulcular epithelium 15.
Initiation of the cellular response:
- Initiation of the host immune reaction to bacteria and their products leads to the activation of the complement system.
- The products of complement system like, C5a act as a chemoattractant for neutrophils. This leads to the recruitment of leukocytes and monocytes in that area.
- Cellular response is characterized by the presence of neutrophils, which are the hallmark of acute inflammatory reaction. Because of increase in vascular permeability, PMN’s emigrate from blood vessels into the connective tissue by a process called transendothelial migration (read ‘Mechanism of transendothelial migration of leukocytes’ in the chapter 6 for more details).
- Activated macrophages produce various chemical mediators, which further intensify the inflammatory reaction. These include IL-1β, IL-6, IL-10, IL-12, TNF-α, MMP, IFN-γ, PGE2.
- They also release chemotaxins like, monocytes chemoattractive protein (MCP), macrophage inflammatory proteins (MIP), RANTES (regulated on activation, normal T-cell expressed and secreted).
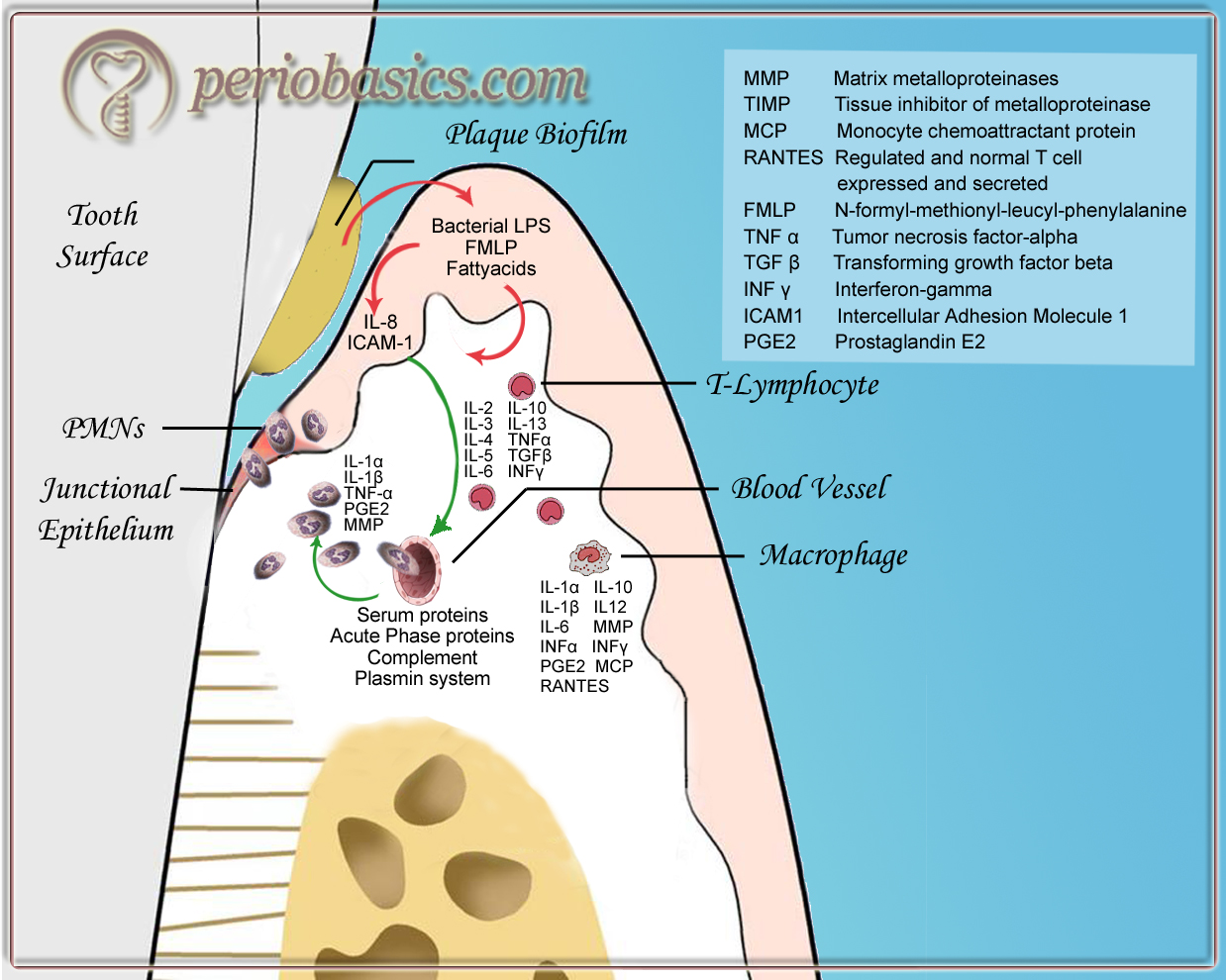
Initiation of connective tissue breakdown:
- As the duration of inflammatory response prolongs, the inflammatory infiltrate is dominated by lymphocytes. Subsets of T-cells, i.e. helper T-cells (T ) and cytotoxic T- H cells (T ) are involved in regulating the immune C responses. They also help in the initiation of B-cell response that leads to the formation of antibodies.
- T-cell mediated response leads to the release of … Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book…….
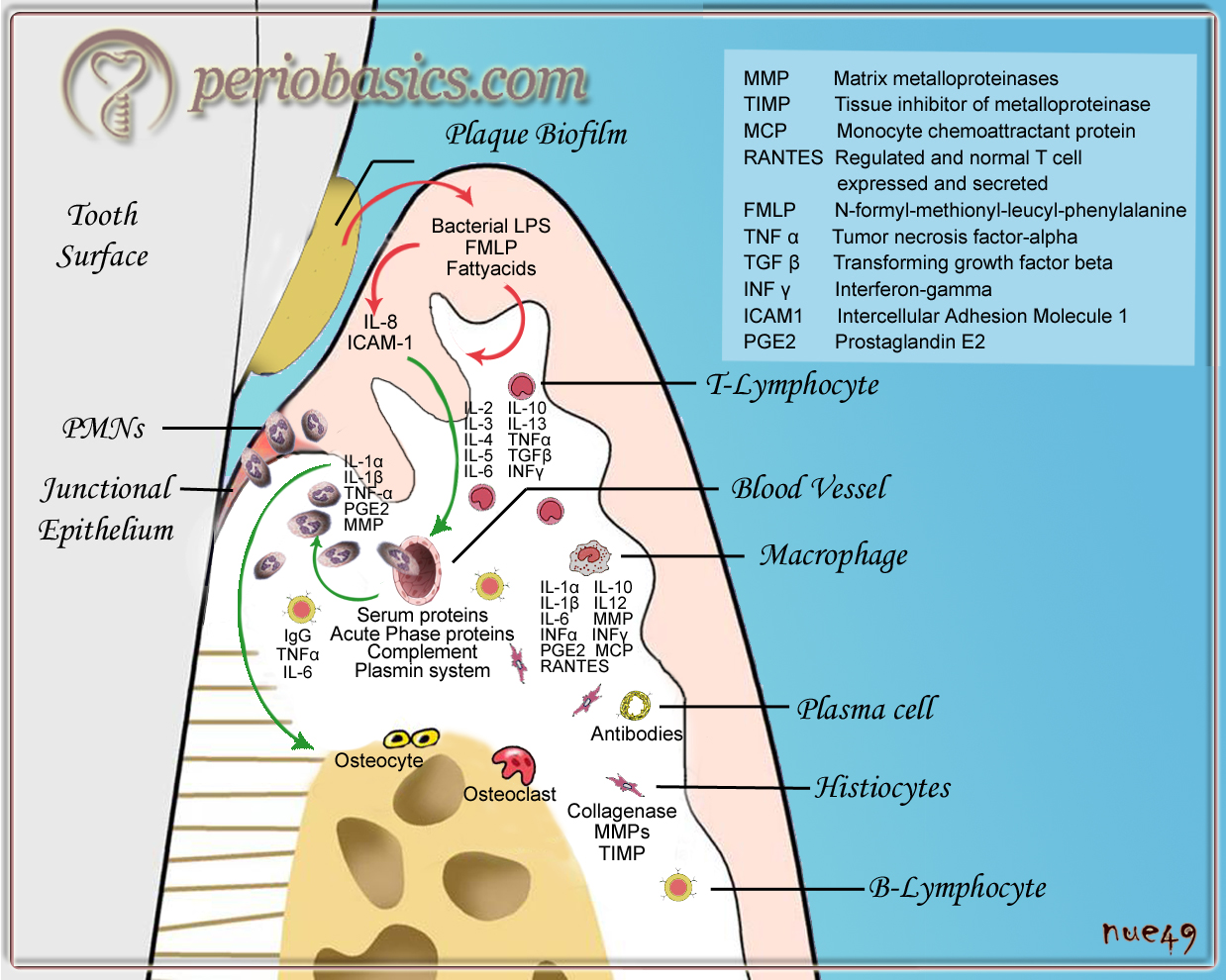
Initial attachment loss:
- This stage is dominated by plasma cells.
- Immunologically active cells infiltrating the connective tissue cause its degradation. The activated macrophages and other cells further elaborate the immune response.
- Immunocompetent cells produce various cytokines, MMPs, PGE2 and TIMPs.
- All these events lead to the disturbed tissue homeostasis and leads to the destruction of connective tissue matrix, bone and collagen fibers. This ultimately leads to the pocket formation and consequently periodontitis.
Immunological mediators and complement components in inflamed gingiva
Immunological mediators:
Before we discuss the immunological mediators in inflamed gingiva, it must be clear that untreated gingivitis may result in periodontitis and the immunological mediators involved both in gingivitis and periodontitis are the same. However, their levels in tissue may vary in both the conditions. As discussed in the previous chapters, inflammatory mediators play a crucial role in acute and chronic inflammation. These include a range of interacting molecules like, the cytokine system, proteinases, proteinase activators, thrombin, histamine, prostaglandins, leukotrienes, tissue and blood factors such as Hageman’s factor, complement and clotting factors. These mediators lead to the initiation and eventually, termination of an inflammatory response to insult. These are present in inflamed gingiva and gingival crevicular fluid (GCF) from diseased sites in high concentrations 16 and their concentration typically decrease, following successful periodontal therapy. In some individuals, the elevated amount of these mediators is released from cells like monocytes, which cause rapid destruction of periodontal connective tissue 1.
During gingival health, a vital balance is maintained between the pro- and anti-inflammatory mediators. During gingival inflammation, the pro-inflammatory cytokines are increased in the gingival tissue. Among pro-inflammatory cytokines, particular attention has been paid to the roles of IL-α, IL-β, IL-6, IL-8, TNF-α and PGE2 in the pathogenesis of periodontal disease. Many investigators have demonstrated that IL-1α, IL-1β, IL-6, IL-8, and TNF-α can be detected in GCF in gingivitis and periodontitis 17-19 and that the cytokine levels in GCF are closely associated with the severity of gingival inflammation and/or periodontal tissue destruction 20, 21.
As already discussed in the previous sections, IL-8 plays a vital role during inflammation. Secreted by a variety of cells, including monocytes, fibroblasts, lymphocytes, and endothelial cells, IL-8 formerly known as neutrophil-activating peptide-1 (NAP-1) is a potent chemotactic factor for leukocytes 22. IL-8 induces neutrophil extravasation and plays a very important role in the accumulation of leukocytes at the site of inflammation 22. IL-8 may also attract T-cells and induce motility in the CD45RO+ yδ and αβ T-cells present in inflamed gingiva 23, 24. The levels of IL-8 have been shown to be elevated at the sites of inflammation as compared to healthy sites 25.
It is well established that IL-1 has important roles in … Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book…….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
TNF-α stimulates the secretion of collagenase by fibroblasts, resorption of cartilage and bone, and has been implicated in the destruction of periodontal tissue in periodontitis 35, 36. LPS is a strong inducer of production of TNF-α by peripheral blood monocytes 37, which in turn leads not only to alveolar bone resorption but also to the enhanced synthesis of collagenase by human gingival fibroblasts. As it is a potent inducer of collagenase secretion by fibroblasts 38, it is implicated in the resorption of cartilage 39 and bone 40, and hence in the destruction of periodontal tissue during periodontal disease 41.
Another important mediator of inflammation is PGE2. It is the product of arachidonic acid metabolism. As it is one of the important mediators of inflammation, investigations have been done to evaluate its role in periodontal tissue destruction during inflammation. Various studies have confirmed that GCF PGE2 levels are elevated in periodontitis as compared to gingivitis 42-44. PGE2 is detected in higher levels in inflamed gingival tissue and GCF, proportional to the severity of periodontal disease 45-47. Some investigations suggested that the GCF PGE2 levels are substantially higher in certain high-risk patients, such as refractory periodontitis, early-onset periodontitis or diabetic patients 48. These investigations have led us to investigate the genetic aspect of periodontal diseases.
MMPs are involved in the maintenance of connective tissue. However, in inflamed gingiva, their levels are increased. They are excreted by a variety of connective tissue and pro-inflammatory cells including fibroblasts, osteoblasts, endothelial cells, macrophages, neutrophils, and lymphocytes. In earlier studies, collagenases had been identified in explanted gingival tissues and their culture fluids 49-51 and in homogenates of gingival biopsies 52. MMPs are classified according to their substrate specificity as collagenases, gelatinases, stromelysins and matrilysins 53. For a detailed description please read “Matrix metalloproteinases and their role in periodontal diseases”.
Complement components in inflamed gingiva:
Shillitoe and Lehner in 1972 54 demonstrated the presence of complement components in GCF. Following their study, many investigations demonstrate that C3 and factor B cleavage fragments are commonly found in GCF and that the relative quantity of C3 fragments correlates with the severity of inflammation and the amount of supragingival plaque 55-59. In addition, C4 cleavage is rarely seen except in the case of localized juvenile periodontitis (LJP).
Genco and co-workers (1974) 60 were first to report the presence of complement proteins in gingival tissue. They used antibodies against C3 and C4 and demonstrated that these proteins could be detected in sections from healthy and inflamed gingival tissue. Further studies investigated the presence of IgG, IgM, and C3 in gingival tissues 61, 62. Studies have shown that diseased gingival tissues (but not healthy tissues) synthesizes IgG, IgA, C3, and C5 63, 64.
Immune response in gingival health
To understand the periodontal immune response in gingivitis and periodontitis let us first try and understand the response in periodontal health. The periodontium is considered healthy in the absence of inflammation. This state is characterized by the absence of an inflammatory infiltrate which can only be seen in subjects practicing extensive mechanical oral prophylaxis. Usually, we have sub-clinical inflammation. One of the most important parts of periodontium, that is a central place for host immune response, is the dentogingival unit. It is the adaptation of the oral mucosa to the tooth surface that comprises of epithelial and connective tissue components. The epithelium is divided into three functional compartments – gingival, sulcular, and junctional epithelium. The connective tissue is divided into superficial and deep compartments. Out of these, junctional epithelium plays most important role in periodontal health and disease states. In healthy state, gingival tissue contains a low number of leukocytes primarily classified as lymphocytes. Various studies have been done to investigate the levels of inflammatory mediators in healthy and inflamed periodontal tissues. Some of them are summarized here,
- In clinically healthy gingival tissues, inflammatory cytokines are present in low quantities, suggesting, cytokines are also prominent factors mediating normal tissue homeostasis 65.
- Low levels of PGE2 have been found at sites free of periodontal inflammation as compared to an inflamed site where their levels are high. PGE2 is considered as a marker of inflammation 16.
- Low or no IL-1β is detected in tissue extracts from healthy sites, whereas its levels are clearly detectable in inflamed gingival sites 66.
- Levels of IL-8 have been found to be increased at healthy sites as compared to the sites with periodontitis. IL-8 is a potent migratory signal for neutrophils to the site of ingress of bacterial products 67.
- On examination of subjects with healthy gingiva and subjects with periodontitis, it has been found that fewer number of cells containing TGF-β1 are found in healthy gingiva 68.
Immune response in gingivitis
As explained in the previous sections, gingivitis starts with the ingress and accumulation of bacteria and their products in the oral sulcular epithelium. The primary response to this is associated with the release of chemical mediators from junctional epithelium which causes recruitment of polymorphonuclear cells in that area. Now, various chemical mediators are secreted by immunocompetent cells during the host-bacterial interactions. The GCF has been used as an important source for the analysis of various enzymes and inflammatory mediators.
Alterations in crevicular fluid levels of … Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book…….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
One experimental gingivitis study showed that the gingivitis was associated with a significant 2.6 fold increase in IL-1β, a 3.1 fold increase in IL-1α and a significant decrease in multiple chemokines as well as MMPs-1, -3 and 13 70. Lactate dehydrogenase (LDH), β-glucuronidase (BG) and arylsulfatase (AS) activity in GCF associated with experimental gingivitis was investigated in one study. Results showed that the LDH concentration in GCF varied minimally during the experiment, while total LDH activity rose slightly over the 4-week period. BG concentration and total activity in GCF rose steadily from baseline to the 3rd week and then either fell or leveled off during the 4th week. AS concentration in GCF rose from baseline to the 2nd or 3rd week and then fell. AS total activity in GCF rose from baseline to the 2nd week and then remained constant. The authors suggested that there may be a homeostatic mechanism in the crevicular environment, which may control ground substance-degrading enzyme activity during experimental gingivitis 71.
Clinical features of gingivitis
The clinical features of gingivitis are a result of histological changes in the tissue due to the release of pro-inflammatory mediators. The initial events in gingivitis are caused due to changes in the gingival vasculature, specifically increased blood flow through dilated capillaries.
Gingival bleeding:
Gingival bleeding is one of the earliest symptoms of gingival inflammation. Bleeding during probing is a very important finding during the routine periodontal examination. It results due to dilation and engorgement of the blood capillaries. The severity of gingival inflammation varies according to the degree of inflammation in the underlying connective tissue. Due to the inflammation, changes are observed in the sulcular epithelium, primarily the widening of intercellular spaces. As the inflammation becomes chronic, ulceration in the sulcular epithelium may be observed. The capillaries engorged with blood become closer to the surface due to ulceration which results in bleeding even by slight provocation. However, it must be remembered that bleeding on probing is not indicative of any form of periodontal disease.
Gingival bleeding may be acute, due to toothbrush trauma, injury due to sharp pieces of hard food, gingival burns due to hot food, chemical injury and necrotizing ulcerative gingivitis. Chronic gingival bleeding is observed in chronic gingival inflammation. Other systemic factors that may result in increased gingival bleeding include deficiency of vitamin C (causes vascular abnormalities), vitamin K (involved in clotting mechanism), platelet disorders (idiopathic thrombocytic purpura), coagulation defects, malignancies (leukemia) and drugs such as salicylates and anticoagulants.
Significance of gingival bleeding:
As already stated, bleeding on probing is considered as one of the first signs of gingival inflammation; it is a simple clinical test for early diagnosis of developing gingivitis. Clinical probing with a periodontal probe should be done carefully by applying appropriate pressure. A detailed description of probing technique has been given in “Art of history taking in periodontics”. As bleeding on probing is commonly present before other visual signs of inflammation, many indices have been developed for the assessment of gingival status based on gingival bleeding. Bleeding on probing is also a good indicator of active or inactive existing periodontal disease. However, it should be remembered that bleeding on probing does not give any indication about the extent of periodontal destruction.

Changes in gingival color:
The color of the gingiva is determined by the vascular supply, degree of keratinization of the overlying epithelium and melanin pigmentation. The normal color of the gingiva is ‘coral pink’. During inflammation, the color of the gingiva becomes reddish pink to bluish pink, depending on the degree of vasodilation and engorgement of blood capillaries. As the gingivitis takes a chronic course, the color of the gingiva becomes ……Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book………. Contents available in the book…….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Local factors:
- Acute gingivitis
- Chronic gingivitis
- Metallic pigmentation
Acute gingivitis may result due to heat burns, chemical injuries, necrotizing ulcerative gingivitis (NUG), or herpetic gingivostomatitis. In heat or chemical induced injuries, gingival redness appears in the localized area, where the insult has taken place. In NUG, the gingival margins have a bright red erythematous appearance. However, in severe acute inflammation, the red color may gradually become dull and whitish gray, which is caused due to tissue necrosis. The necrosed area can be demarcated from the adjacent gingiva by a thin, sharply defined erythematous zone. In herpetic gingivostomatitis, there is diffused redness of the gingiva.
In chronic gingival inflammation, the gingiva is marked by reddish to bluish color change. This may be attributed to vascular proliferation and reduction in the degree of keratinization.
Various heavy metals may impart different color to the gingiva. It should be noted that gingival pigmentation due to heavy metals is not a result of systemic toxicity. It occurs only in the areas of inflammation, where the increased permeability of the blood vessels allows seepage of metal ions into the surrounding tissue. Various metals with their corresponding gingival pigmentation are,
- Lead: Bluish-red, deep blue or gray (Burtonian line).
- Bismuth: Black line.
- Mercury: Black line.
- Arsenic: Black line.
- Silver: Violet marginal line.
- Amalgam: localized bluish-black areas.
Systemic factors:
The systemic factors which may cause gingival pigmentation may be endogenous or exogenous in origin.
Endogenous factors:
- Addison’s disease: increased melanin pigmentation.
- Peutz-jeghers syndrome: increased melanin pigmentation.
- Albright’s syndrome: increased melanin pigmentation.
- Jaundice: yellowish color due to deposition of bilirubin.
- Hemochromatosis: bluish-gray due to deposition of iron.
- Drugs: Chloroquine (slate gray), minocycline (brown), chlorpromazine, zidovudine, ketoconazole, methyldopa, busulphan.
- Diabetes
- Pregnancy
- Blood dyscrasias
- Hyperthyroidism
Exogenous factors:
- Tobacco/smoking: grayish color due to increased melanin pigmentation.
Gingival contour:
Healthy gingiva has a scalloped and knife-edged contour. The shape of the interdental papilla in the anterior areas is pointed and pyramidal, whereas in the posterior region, it is tent-shaped, filling the area. The contour of the gingiva changes in various clinical conditions. In acute or chronic inflammation, the gingival margins may be rolled or rounded. In the gingival enlargement, the interdental papillae may become bulbous. In necrotizing ulcerative gingivitis, papillae may be cratered. There are two specific forms of gingival contours which have been named as Stillman’s cleft and McCall’s festoons.
Stillman’s cleft:
Stillman’s cleft is a mucogingival triangular-shaped defect on the buccal or labial surface of tooth/teeth with unknown etiology and pathogenesis. These are apostrophe-shaped indentations which extend from and into the gingival margin along the root surface. Most commonly these are observed on the labial or the buccal aspect. The margins of the cleft are rolled underneath the linear gap in the gingiva and the remainder of gingival margin is blunt in contour. Originally, Stillman described these clefts to be a result of occlusal trauma. The cleavage may be simple (in a single direction) or compound (in more than one direction).
McCall’s festoons:
These are “life-saver” shaped, semilunar enlargements of the marginal gingivae primarily on the labial surfaces of the anterior and premolar teeth. These were named after John Opple McCall, who, along with Paul R Stillman, believed occlusal traumatism to be their primary etiology.
Gingival consistency:
As described earlier, the consistency of the gingiva depends on the underlying changes in the connective tissue. In acute gingivitis, the gingiva becomes edematous, demonstrating a soft consistency, whereas, in chronic gingivitis, the gingiva demonstrates soggy puffiness that pits on pressure or firm, leathery consistency. In chronic gingivitis, the gingiva may show both edematous and fibrotic consistency, depending upon the relative predominance of the destructive (edematous) or reparative (fibrotic) component.
Surface texture of the gingiva:
The normal surface texture of the gingiva is stippled with an ‘orange peel’ appearance. Stippling is best viewed by drying the gingiva. Stippling is commonly observed on the attached gingiva and is absent on the marginal gingiva. The central portion of the interdental papillae is usually stippled, but the marginal borders are smooth. Furthermore, pattern and extent of stippling vary among individuals and different areas of the same mouth (read more in the “Periodontium in health”). During inflammation of the gingiva, stippling is lost and the gingiva appears smooth and shiny. However, it must be remembered that the surface texture of the gingiva is not considered as a reliable indicator of gingival inflammation. These changes are also seen in atrophic gingivitis and chronic desquamative gingivitis. In the drug-induced gingival enlargement, the nodular surface texture of the gingiva can be seen. In hyperkeratosis, leathery surface texture of the gingiva is observed.
Position of the gingival margin:
The normal position of the gingival margin is 1-2 mm above the cementoenamel junction. The position of the gingival margins may move in the coronal or the apical direction in different conditions. In the gingival enlargement, the position of the gingival margin moves in a coronal direction, whereas in recession, the gingival margin moves in an apical direction.
Conclusion
Gingivitis is one of the most common lesions encountered in the clinical setting and may be the first sign in many types of periodontal diseases. There are many clinical conditions which have gingivitis as their initial clinical manifestation. A clinician should have a thorough knowledge regarding the development of gingivitis because it has important diagnostic relevance in early detection and prevention of various periodontal diseases.
References
References are available in the hard-copy of the website
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.