Introduction
A furcation (or furca) is the area of a tooth where the root divides from the common root trunk into a bifurcation or trifurcation. Furcation involvement in posterior teeth is the result of progressive periodontal breakdown due to inflammation. It is important to determine the extent of furcation involvement to make an appropriate diagnosis and develop a treatment plan. Furcation involvement worsens the prognosis of the tooth because long-term studies indicate that teeth with furcation involvement are the teeth that tend to be lost over time. In a study, Hirschfeld and Wasserman (1978) 1 reported that percentage of tooth loss in furcation-involved molars was 31.4% as compared to 4.9% in single-rooted teeth after a mean maintenance period of 22 years. Similarly, McFall (1982) 2 reported that the frequency of tooth loss with furcation-involved teeth was 57% as compared to 7% for single-rooted teeth.


The access to the furcation area is difficult both for the dentist and patient, and their treatment constitutes an enormous challenge. The treatment of teeth with furcation involvement ranges from thorough debridement to regenerative procedures and, if the lesion progresses, to extraction. In the following discussion, we shall discuss in detail the etiology of furcation involvement and its potential treatments.
Anatomy of furcations
Furcations present very unusual challenges for instrumentation due to their anatomical features. It is important to understand the anatomical features of furcation to appropriately treat these difficult to reach areas. The portion of a multi-rooted tooth apical to the cementoenamel junction (CEJ) is called root complex. It can be further divided into root trunk and root cones. Root trunk is the undivided portion of the root complex. The height of the root trunk is the distance between CEJ and line where root cones start. The root trunk height may vary from surface to surface on a molar or premolar. The root cones start at the furcation point from where they may take various shapes diverging from the root trunk. The furcation fornix is referred to as the roof of the furcation area and furcation entrance is the transitional area between the divided and undivided roots. Root divergence is the degree of separation of roots and coefficient of separation is the length of root cones in relation to the length of the root complex.
The roots may have different shapes and may be completely or incompletely ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Maxillary premolars:
The root of the maxillary first premolar is usually bifurcated in the apical or middle third making facial and palatal roots. When viewed from the mesial aspect, a longitudinal groove extends from the contact area to the bifurcation. The mean distance of the furcation from CEJ for maxillary first premolar is ~7 mm with a furcation width of approximately 0.7 mm.
Maxillary first molar:
The maxillary first molar is the largest tooth in the maxillary dental arch. It has three roots, mesiobuccal, distobuccal and palatal root. The palatal root is the longest, the mesiobuccal root is not as long, but it is broader buccolingually, the distobuccal root is the smallest of all the three roots. The average root trunk length from the cervical line to the furcation area is around 4 mm. Usually, there is a deep developmental groove which extends on the buccal surface of the root trunk from the furcation area toward the cervical line, where it terminates in a shallow depression or it may extend slightly on the enamel surface at the cervix. The buccal furcation entrance is narrower than the distal and mesial furcation entrances. The distobuccal root is narrower than the other two roots. When seen from the mesial surface, the mesiobuccal ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
There are three furcation entrances on a maxillary first molar and these are located at varying distances from the CEJ. The distance of the mesial furcation entrance from CEJ is around 3 mm, while that of buccal and distal furcations from CEJ is 3.5 and 5 mm, respectively 3, 4. It indicates that the furcation fornix is inclined in the mesiodistal plane and the mesial furcation entrance is closer to CEJ as compared to the distal entrance.
Maxillary second and third molars:
In general, the overall size of maxillary second molar is smaller than the first molar and larger than the third molar. The root trunk length of the second maxillary molar is more than the first molar and hence the respective furcation entrances are farther from CEJ as compared to the first molar. The degree of root separation of the second molar is less than the first molar and that of the third molar is less than the second molar. All the depressions found on the root surface of the ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Mandibular first molar:
The mandibular first molar has two roots, a mesiodistally flattened mesial root and a mostly straight and more rounded distal root 5. The mesial root is curved mesially from cervical third to the middle third portion. The distal root is less curved and its axis is in the distal direction from the root trunk to the apex. Both mesial and distal roots are wider mesiodistally on the buccal aspect as compared to the lingual aspect. The point of bifurcation is present approximately 3 mm below the CEJ on the buccal aspect and 4 mm below the CEJ on the lingual aspect. Thus, the furcation ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Mandibular second and third molars:
The root trunk length of mandibular second molar is more than the first molar. Root divergence of mandibular second molar is less than the first molar. The root trunk of both first and second molar has a depression between the bifurcation and cervical line. The shape of mandibular third molar varies considerably from individual to individual. The mesial and distal roots may have a definite bifurcation point or they may be fused for all or a part of their length.
Etiology of furcation involvement
The most common etiology of furcation involvement is bacterial plaque causing inflammation in periodontal tissues. Extension of inflammation leads to progressive loss of soft and hard tissues in the bifurcation and trifurcation of posterior teeth. Other predisposing and contributing factors which facilitate furcation involvement include toothbrush trauma causing recession and loss of attachment, trauma from occlusion, endodontic lesions that get access to furcation area, the thickness of investing alveolar process, root fracture and iatrogenic factors. A tooth may also be predisposed to furcation involvement due to anatomical factors and root fracture involving furcations 6. Following is the detailed description of these factors,
Extension of inflammatory periodontal diseases into furcation:
The plaque-induced inflammation causes the destruction of collagen fiber attachment of gingiva and alveolar bone. Furcation involvement is primarily due to the rootward extension of the periodontal pocket in the region of furcation. The resolution of ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Trauma from occlusion (TFO):
TFO is a predisposing factor for a more rapid involvement of furcation in inflammatory periodontal diseases. It has been well established that in the absence of inflammation, TFO causes alterations in the alveolar bone, cementum, and PDL but does not initiate the attachment loss. However, TFO combined with deeper inflammation in close proximity to furcation results in more rapid loss of attachment than from inflammation alone. One of the factors contributing to the formation of isolated furcation defects in molars may be a greater susceptibility of molars to traumatic forces. TFO is particularly considered as a contributing factor in case of furcation involvement with crater-like or angular deformities in the bone and especially when the bone loss is confined to one of the two roots.
Cervical enamel projection:
The cervical enamel projection (CEP) is an enamel projection, which extends from the CEJ to furcation. Masters and Hoskins (1964) 7 reported the incidence of CEPs in extracted human teeth and suggested their possible implication in isolated furcation involvement. They can be classified on the basis of their proximity to furcation entrance as,
Grade I – The enamel projection extends from the CEJ of the tooth toward the furcation entrance.
Grade II – The enamel projection approaches the entrance to the furcation. It does not enter the furcation, and therefore, no horizontal component is present.
Grade III – The enamel projection extends horizontally into the furcation.
The prevalence of CEP’s varies significantly from study to study, however, overall mean values have a range from 8.6 to 32.6% in molars 7-9. A higher prevalence of CEPs has been found in the mandibular molars than in the maxillary molars. Further, the prevalence is highest for mandibular and maxillary second molars. Grade II enamel projection has a higher prevalence as compared to ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Pulpal-periodontal diseases:
There is a high percentage of molars with patent accessory canals that open in their furcation areas 11-15. It is one of the co-factors contributing to the development of furcation lesion. The presence of accessory canals in the furcation area may easily extend the endodontic infection in the furcation area and may result in bone loss in furcation. In one study, the prevalence of accessory canals in the furcation region of molars has been found to be 28.4%. Out of total samples, accessory canals in the furcation area were demonstrated in 29.4% of mandibular molars, and 27.4% of maxillary molars 16. With no apparent periodontal involvement, the endodontic lesion gets access to the furcation by accessory canals. The endodontic treatment of tooth resolves the periodontal problem also. Regeneration of new intrafurcal bone and attachment can be expected in such cases. If there is an accumulation of plaque in the furcation area adjacent to endodontic sinus tract, the lesion becomes endo-perio lesion. If the furcation lesion is detected in ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Thickness of investing alveolar process:
During the inflammatory process, the thick alveolar process may predispose to the formation of deep horizontal and vertical defects without soft tissue recession, whereas thin bone is commonly associated with recession, which may result in easier access to the furcation.
Root fracture:
A rapid localized bone loss is often seen in association with vertical root fracture. In case of vertical root fracture involving trunk of the root, frequently its extension to furcation area is found. It may result in the rapid formation of isolated furcation lesion. The prognosis of such teeth is poor and frequently, tooth loss results.
Iatrogenic factors:
The development of furcation lesions has also been demonstrated due to inappropriate treatments. Overhanging restorations result in harboring of plaque resulting in inflammation and thus initiating the development of a furcation lesion. It has been observed that molars with restorations have a higher prevalence of furcation involvement than the non-restored molars.
Prevalence of furcation lesions
The furcation lesions are most commonly seen in maxillary and mandibular first molars 17. This is because of their anatomy and the fact that these teeth suffer the longest exposure to plaque associated insult throughout the patient’s lifetime. The incidences of furcation involvement increase with increasing age. The chances of tooth loss are increased following furcation involvement 18. In lower molars, the buccal furcation is most commonly involved, while in the upper molars the buccal furcation is likewise usually the most commonly involved, followed by ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Diagnosis of furcation involvement
The diagnosis of furcation involvement is made on the basis of patient’s clinical history, thorough clinical examination, radiographic examination, consultation with other specialists when indicated and if necessary, laboratory tests. A curved explorer or Naber’s probe and bone sounding are used to make a clinical diagnosis of furcation involvement 20.
The prognosis of the tooth is established only after the exact condition of furcation is known. There are various factors which are considered while making a diagnosis of furcation involvement and establishing the prognosis of the involved tooth. These include 21,
- Root trunk length.
- Size of the furcation.
- Root separation and divergence.
- Root fusion.
- Root concavity.
- Crown root ratio of the tooth.
- Occlusal interferences and trauma from occlusion.
- Tooth mobility.
- The ease with which hygiene of the affected furcation can be maintained.
- The capacity of the patient to maintain optimum hygiene.
- The extent of furcation disease can be determined by evaluating
- Vertical bone loss.
- Horizontal bone loss.
- Both vertical and horizontal bone loss.
- Out of horizontal and vertical bone loss parameters, the horizontal bone loss is more commonly used.
Classification of furcation involvement
Various classifications have been proposed historically to describe the horizontal and/or vertical component of furcation involvement. The furcation involvement has been classified on the basis of involvement of horizontal component or vertical component or both. There are more than 19 classification systems proposed to classify furcation involvement. All these classification systems have been given in the hard-copy of the website, Periobasics: A textbook of Periodontics and Implantology.
Management of furcation involvement
As already mentioned furcations are areas of complex anatomic morphology 41 and are difficult to debride by routine periodontal instrumentation 34. Presently, there is no uniformity in the terms used to describe various treatments for teeth with furcation involvement. Various terms have been used to describe ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Furcationplasty:
The reshaping of alveolar bone in the furcation area is known as furcationplasty. Furcationplasty can be applied to the buccal and lingual furcation areas. If the same procedure is carried out on the tooth structure, it is called as odontoplasty.
Root amputation:
Root amputation is characterized as removal of a root without removal of the overhanging portion of the crown 42.
Root resection:
Root resection generally indicates the removal of a root without any information on the crown of the tooth 42.
Root separation:
Root separation is indicated as the sectioning of the root complex and the maintenance of all roots 42.
Bicuspidization:
This is the procedure done for mandibular molars where a single molar tooth can be converted into two bicuspids by retaining both mesial and the distal root.
Hemisection:
Hemisection is defined as the removal of half of a tooth performed by sectioning the tooth and removing one root. It is frequently used with reference to lower molars 42.
Tunneling procedures:
The tunneling procedure is the intentional creation of a class III furcation with its entrance accessible for oral hygiene procedures.
Treatment of Grade I furcation involvement
Maintenance of adequate oral hygiene is required for preventing furcation lesion from progression. The patient should be educated about the maintenance of good oral hygiene and should be re-evaluated at a frequent interval. For Grade I furcation involvement, following treatment modalities are usually employed,
- The furcation can be debrided with or without open flap debridement but with no modification of the furcation.
- Furcationplasty and/or odontoplasty can be done to eliminate the opening of the furcation. The procedure is usually indicated in incipient lesions with very well defined cementoenamel junctions. It results in the elimination of the bacterial reservoir in the grooves of the furcation pillars. The main disadvantages of this procedure are increased dentinal sensitivity and appearance of secondary caries. Further, this treatment alone may not stop disease progression and the patient should be motivated to maintain good oral hygiene.
- Another treatment is covering the furcation with periodontal plastic surgery. Connective tissue grafts and coronally positioned flaps can be employed to cover the ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Treatment of Grade II furcation involvement
Grade II or Cul-de-sac like furcation defect can be treated by both regenerative and resective procedures.
Open or closed flap debridement without modification of the furcation has been shown to be not very effective in the management of Grade II furcation defects. Schroer et al. (1991) 44 in their study on 25 furcation sites with grade II defect in 15 patients compared scaling and root planing to open flap debridement. The results of the study demonstrated a reduction in probing depth in both groups at the deepest vertical site in the furcation. On the other hand, Kalkwarf et al. (1988) 45 reported a ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Guided tissue regeneration has been shown to be an effective procedure for the treatment of Grade II furcation defects 46. The procedure has been shown to result in the filling of the defect with the clinical closure of the furcation. However, it should be remembered that spontaneous regeneration following meticulous debridement is also possible. The procedure can also be done in combination with enamel matrix proteins or growth factors which have provided a new focus for this kind of treatment. The main problem associated with this procedure is exposure of the surgical membrane or infection 47.
Tunneling procedure is recommended mainly to treat advanced Grade II and Grade III lesions 17, 48. In this procedure, bone is reshaped to obtain a scalloped morphology and the soft tissues are apically positioned. The procedure results in exposure of tooth furcation to the oral environment which can be easily cleansed by the patient. It must be made sure that space obtained under the roof of furcation should be adequate enough to allow proper plaque removal 41. Both short term and long term results of this therapy have reported variable results with this therapy. Hamp et al. (1975) 25 carried out tunneling procedure on 7 molars with degree III furcation involvement. Five year follow-up results demonstrated that 4 out of 7 teeth had evidence of carious lesions. The authors suggested unfavorable results of this therapy. In another study, Little et al. (1995) 49 followed 18 teeth with class II or III molar furcations that underwent tunneling procedures. The results of the study demonstrated that crestal bone levels and ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Treatment of Grade III furcation involvement
There are many factors which determine the clinician’s decision to choose one treatment plan over another when confronted with a Class III furcation invasion. These factors may be classified into three categories,
Local factors:
Tooth anatomy.
Tooth mobility.
Crown root ratio.
Severity of attachment loss.
Inter-arch and intra-arch occlusal relationship.
Cost-benefit ratio for retaining a portion of the root.
Patient-related factors:
Health of a patient.
Importance of the tooth to the patient.
Costs and time factor.
Clinician-related factors:
Selection of the case.
Diagnostic and treatment planning skills.
Awareness of therapeutic options.
Skill of the clinician.
Tooth anatomy is the primary determinant in establishing treatment planning for grade III furcation involvement. The divergence of root cones, their length, and remaining bone support should be considered to establish the treatment plan. The crown root ratio affects the long-term stability of the preserved portion of the tooth. As already stated, the severity of attachment loss determines the portion of the tooth, which can be saved and the portion which should be removed. The root cone with adequate bone support should be saved so that it can withstand occlusal forces. Along with this, the saved root cone should be placed in the occlusal plane so that after placement of fixed prosthesis, adequate inter-arch, and intra-arch occlusal relationship can be maintained. The patient should be well motivated to keep the involved area free of plaque and inflammation. Following are the treatment procedures considered while making a treatment plan for maxillary and mandibular molars with grade III furcation involvement,
Mandibular molars:
Tunneling procedure
Root separation
Bicuspidization
Hemisection
Root amputation
Maxillary molars:
Root amputation
Hemisection
Trisection
Tunneling procedure:
As described earlier in the management of grade II furcations, the procedure allows “through and through” cleansing of the furcation where root anatomy allows and is indicated in highly motivated patients.
Root separation:
Root separation involves sectioning of the root complex and maintenance of all the roots. In teeth with short root trunk length, there is early involvement of furcation. These teeth are indicated for this procedure because following the procedure, there remains a good amount of supporting bone around the root cones. On the other hand, in teeth with ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
The divergence of the root cones is another important factor to be considered while planning this treatment. This treatment is suitable in cases where root divergence is more i.e. roots are wide apart. It allows appropriate rehabilitation of each root cone. In cases where roots divergence is less, orthodontic root movement may be necessary to create an appropriate space between the root cones.
Root length and shape determine the stability of root cones after root separation. Longer the roots, more stable they are under occlusal load. Short and small roots exhibit increased mobility following separation and thus are not good abutments for subsequent prosthetic restoration.
While planning for root separation it must be made sure that the root cones are not fused. It can be determined by clinical and radiographic examination. It may be difficult to ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
It must be made sure by clinical and radiographic examination that following root separation each root cone has an adequate amount of bone support after the procedure.
Bicuspidization:
Bicuspidization is one of the procedures for the management of furcation involvement in mandibular molars. This procedure is done in lower molars with well defined and well separated mesial-distal roots. The procedure involves root canal treatment of the involved tooth and dividing the molar into two parts each having an individual crown. Another ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
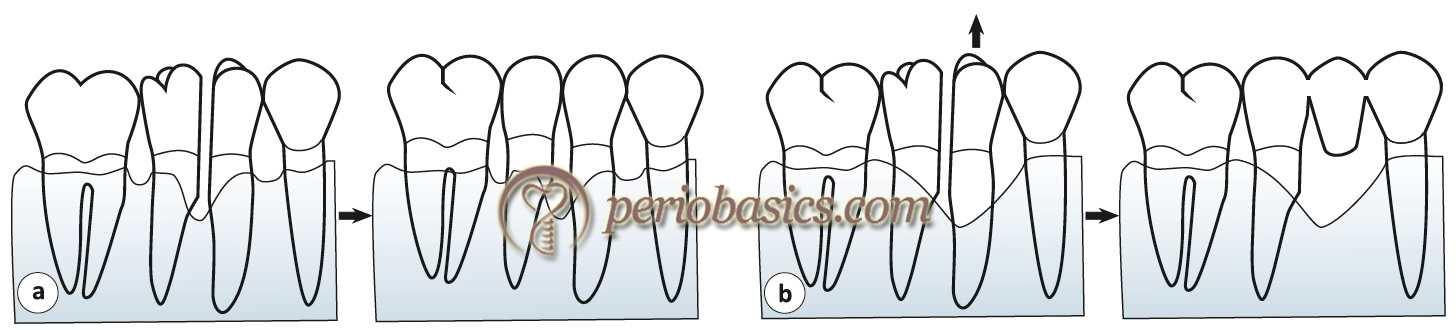
Hemisection:
As already stated, hemisection involves removing signifi-cantly compromised root structure and the associated coronal structure through deliberate excision 51. The term hemisection has been used interchangeably with root resection 52. The procedure is done where only one root of a multi-rooted tooth is affected and the surviving root is structurally capable of supporting a dowel and core restoration. In addition to this, the surviving root should be aligned so as to provide a proper ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
However, it is preferable to go for endodontic treatment of the involved tooth before this procedure to avoid intrapulpal dystrophic calcification and postoperative tooth sensitivity 60. For an adequate vision of the furcation, the mucoperiosteal flap is raised. Removal of facial or palatal bone may be required to adequately expose the root to be removed. A fissure or cross-cut fissure carbide bur at high speed is then applied just below the contact point, directing it towards the furcation. The appropriate orientation of the bur during resection is essential to accurately cut the involved root cone. During hemisection of mandibular molars, a vertical cut is placed which passes through buccal and lingual develop-mental grooves, through the pulp chamber and the furcation.
After carefully sectioning the tooth, the damaged root is removed. To allow appropriate ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Root amputation:
The procedure involves removal of the root without removal of the overhanging portion of the crown. The procedure is indicated in patients who are capable of maintaining good oral hygiene and the tooth is also prosthetically maintainable for a relatively long period. In maxillary molars with furcation involvement, this procedure is done when one root is untreatable and two roots have adequate bone support and the crown does not require a prosthetic restoration. In mandibular molars, the procedure involves removal of one root with retaining the complete crown of the tooth. The area under the crown from where the root has been removed should be made self-cleansable by the patient and should allow adequate plaque removal.
Trisection:
Trisection 61 is done in cases with grade III furcation involvement in maxillary molars (primarily first molar) with long and divergent roots. Before going for the procedure, the tooth should be evaluated for the long-term stability of each root cone under occlusal load.
Post-treatment maintenance of furcation
Home care by the patient plays a vital role in the overall prognosis of the treated tooth. The interproximal furcation is best maintained by an interdental brush whereas facial and lingual furcations are better maintained by end tuft brush, rubber tip stimulator, or toothpick-in-holder. The patient should be trained regarding the appropriate usage of these plaque control measures. In case of tunnel preparation, the interdental brush of appropriate size should be passed through the ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Literature review
It is a well-accepted fact that furcation involvement is associated with early tooth loss. Studies have compared changes in clinical attachment levels in areas with furcation involvement following open flap debridement and guided tissue regeneration (GTR) procedures. Many systemic reviews have concluded that GTR procedure results in significant attachment gain as compared to open flap debridement 62-66. Further, it has been stated that probing depth reduction was more with all barrier types in GTR procedure as compared to open flap debridement. A retrospective study 67 was done to analyze the factors influencing the treatment decisions for periodontitis-affected teeth and the long-term outcome of these treatment decisions. The authors stated that various treatment modalities for molars with furcation involvement are selected based on the depth of furcation involvement.
The shallow defects can be treated with non-surgical/surgical scaling and root planing with or without furcationplasty whereas deeper defects may require treatments like tunnel preparation, root resection, regenerative procedure or tooth extraction. Factors affecting decision-making for treatment of molars with furcation involvement include tooth mobility, tooth position, lack of antagonist tooth, the degree of furcation involvement and remaining bone support. The results of the study showed that ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
Chen et al. (2013) 68 in a systematic review assessed the evidence on the efficacy of GTR with or without osseous grafting for the treatment of Class II furcation defects. The studies included in this systematic review were analyzed for furcation closure rate, horizontal attachment level gain (HAL), vertical attachment level gain (VAL), horizontal bone fill (HBF), and vertical bone fill (VBF). The results indicated that GTR + bone graft was the most effective therapeutic approach in the treatment of Class II furcation defects. The mean difference between VAL gain in mandibular molars defects between GTR and open flap debridement (OFD) was 1.02 mm (in favor of GTR). The VAL gain for GTR + bone graft and OFD was 1.53 mm (in favor of GTR + bone graft). Hence, it was concluded that in grade II furcation defects, GTR and bone grafting results in better outcomes as compared to OFD.
Another recent systematic review by Avila-Ortiz et al. (2015) 69 analyzed the results of various studies on the outcome of surgical periodontal therapy on furcation defects. The review included 150 articles, of which six were systematic reviews, 109 were clinical trials, 27 were case series, and eight were case reports. The authors concluded that regenerative therapy is predictable in ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ……… Contents available in the book ………
A retrospective study 70 investigated factors affecting treatment decisions and outcome of root resected molars using a nationwide population-based dataset in Taiwan. The results of the study demonstrated 91.1% overall survival rate of root-resected molars. Patients with advanced age (>74 yrs) had 3.33 times higher rates of molar extraction as compared to younger patients. The authors suggested that patient-related factors such as living district, urbanization level, availability of medical institution, and monthly income should be considered while making the decision for root resection.
The presently available evidence suggests that multi-rooted teeth with furcation involvement can be maintained in the oral cavity for a reasonably long duration of time with appropriate nonsurgical or surgical periodontal therapy, provided they are free of plaque and are kept under regular observation.
Conclusion
Similar to all periodontal therapies, the primary aim of non-surgical or surgical periodontal therapy in the furcation areas is arresting the disease process (inflammation and infection), restoring the lost tissues and ultimately, maintaining the teeth in health and function with appropriate esthetics. There are multiple factors which should be taken into consideration while making a decision regarding the treatment of teeth with furcation involvement. These factors include local factors related to the involved tooth, patient-related factors and clinician-related factors. Initial furcation involvement can be effectively treated with adequate plaque control and scaling and root planning, while grade II and III furcations require surgical management. Presently available regenerative therapies have demonstrated good prognosis when used in grade II and III furcation involvement. However, more clinical data is required for the determination of prognosis for teeth with advanced furcation involvement.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.