Introduction
Since the introduction of the concept of osseointegration, remarkable changes have taken place in implant dentistry. Bone quality and quantity plays an important role in the long-term success of implant therapy. Bone is a dynamic biological tissue composed of metabolically active cells that are integrated into a rigid framework. A lot of research work has taken place to determine the success of implants placed in different quality and quantity of bone. Primary stability of the implant has been proposed to be the most important factor responsible for the success of implant therapy, which is primarily determined by the density of the bone. A detailed knowledge of different aspects of bone is essential for long-term implant success. In the following sections, we shall study in detail the bone considerations in implantology.
Biological aspect of bone
Bone is a dynamic tissue. The cellular components of bone consist of osteogenic precursor cells, osteoblasts, osteoclasts, osteocytes, and hematopoietic elements of bone marrow 1. The bone is covered by periosteum, a layer known as the mother of bone. The periosteum is a tough, vascular layer of connective tissue that covers the bone but not its articulating surfaces. The thick outer layer, termed the “fibrous layer,” consists of irregular, dense connective tissue. A thinner, poorly defined inner layer called the “osteogenic layer” is made up of osteogenic cells. The endosteum is a single layer of osteogenic cells, lacking a fibrous component 2.
Osteoblasts are involved in bone formation, osteoclasts in bone resorption and osteocytes are mature osteoblasts trapped within the bone matrix. Primarily, there are three types of bone: woven bone, cortical bone, and cancellous bone 1.
Woven bone is composed of randomly arranged collagen bundles and irregularly shaped vascular spaces lined by osteoblasts. It is formed during embryonic development, during fracture healing (callus formation), and in some pathological states such as hyperparathyroidism and Paget’s disease.
Cortical bone/compact/lamellar bone is remodeled from woven bone by means of vascular channels that invade the embryonic bone from its periosteal and endosteal surfaces. It is well ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……….

Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Cancellous bone /trabecular bone lies between cortical bone surfaces and consists of a network of honeycombed interstices containing hematopoietic elements and bony trabeculae. The trabeculae are oriented in such a way that they provide the best support to the forces exerted on the bone.
Resorption after tooth extraction
After tooth extraction, there is bone remodeling which involves the osteoclastic resorption of the residual alveolar ridge. Bone resorption is particularly more on the labial wall as well as there is bone deposition within the extraction socket. During the first 3 months, the rate of bone resorption is highest which gradually reduces after 6 months. Remodeling is generally complete and stabilized after 1-2 years 3. The rate of bone resorption in the mandible is 3-4 times higher than in the maxilla.
The bone resorption pattern is different in maxilla and mandible. In the maxilla resorption of the alveolar ridge occurs mainly on the buccal aspect. This is because of the reason that the buccal cortical bone of the maxilla is thinner as compared to the palatal bone. So, the remodeling of the maxilla is in a centripetal fashion which makes the maxilla smaller with due course of time. In case of the mandible, the buccal cortical plate is thinner than the lingual cortical plate in all areas except in the molar region. So, bone resorption in the mandible occurs primarily lingually in the premolar areas and buccally in the molar segments. Thus, this kind of resorption in maxilla and mandible make maxilla smaller than the mandible with due course of time.
Available bone
The availability of sufficient bone is a must for implant placement. If the bone is insufficient, bone augmentation procedures are carried out. Various classifications have been proposed to classify the available bone both quantitatively and qualitatively.
Based on the volume of the bone available following classifications have been proposed,
Atwood’s classification
Atwood (1979) 4 proposed a classification for the edentulous mandible. In this classification system, ridge resorption in a horizontal direction was considered. Measurements were made in a cross-section of the mandible at the site of the central incisor. His classification of resorption stages is as follows:
Class I: Tooth bearing alveolus.
Class II: Alveolus after extraction.
Class III: High alveolar process.
Class IV: High, narrow alveolar process.
Class V: Rounded flat alveolar process.
Class VI: Concave flat alveolar process.
Out of these six classes, Class III and above actually represent the stages of bone resorption.
Seibert’s classification
Seibert (1983) 5 classified ridge defects based on the location of the deformity.
Class I ridge defects
It involves bone loss in the buccolingual width only.
Class II ridge defects
It involves loss in the apicocoronal height only.
Class III ridge defects
It is a combination of both buccolingual and apicocoronal loss (both width and height).
Cawood and Howell’s classification
Cawood and Howell (1988) 6 also gave a classification of the resorbed maxilla and mandible. In their study published in 1988, it was found that the shape of the basilar process of the mandible and maxilla remains relatively stable, whereas changes in the shape of the alveolar process are significant in both the vertical and horizontal axis and follow a predictable pattern. They proposed the following resorption stages:
Class I: Dentate ridge.
Class II: Ridge immediately after extraction.
Class III: Broad and rounded ridge with adequate height and width.
Class IV: Knife-edge ridge with sufficient height, but insufficient width.
Class V: Flat ridge with insufficient height and width.
Class VI: Depressed ridge with a cup-shaped surface.
Fallschssel’s classification
Fallschssel’s (1986) 7 classification is based on the examination of 19 skulls. The classification refers only to the shape of the alveolus in the canine and in the incisor region of the edentulous maxilla. Therefore, practical application is limited.
Class I: Dentulous ridge.
Class II: Wide high alveolar process.
Class II: Narrow high alveolar process.
Class III: Sharp high alveolar process.
Class IV: Wide alveolar process with reduced height.
Class V: Completely resorbed alveolar process.
Lekholm and Zarb classification
Lekholm and Zarb in 1985 8 gave a new classification for various degrees of atrophy for both mandible and maxilla.
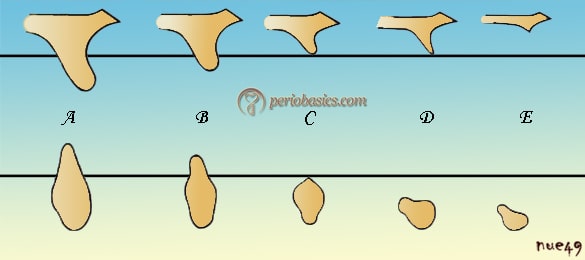
A: Virtually intact alveolar ridge.
B: Minor resorption of the alveolar ridge.
C: Advanced resorption of the alveolar ridge to the base of the dental arch.
D: Initial resorption of the base of the dental arch.
E: Extreme resorption of the base of the dental arch.
(The line in the diagram represents the boundary between the alveolar ridge and the base of the dental arch.)
Misch and Judy classification
In 1985, Misch and Judy proposed a classification system for the available bone with treatment options for each category. This classification system is one of the most commonly used systems for classifying bone volume. For the ease of understanding, they have based their classification system on Kennedy’s classification for ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……….
The Kennedy-Applegate-Fiset Classification System for partially edentulous arches,

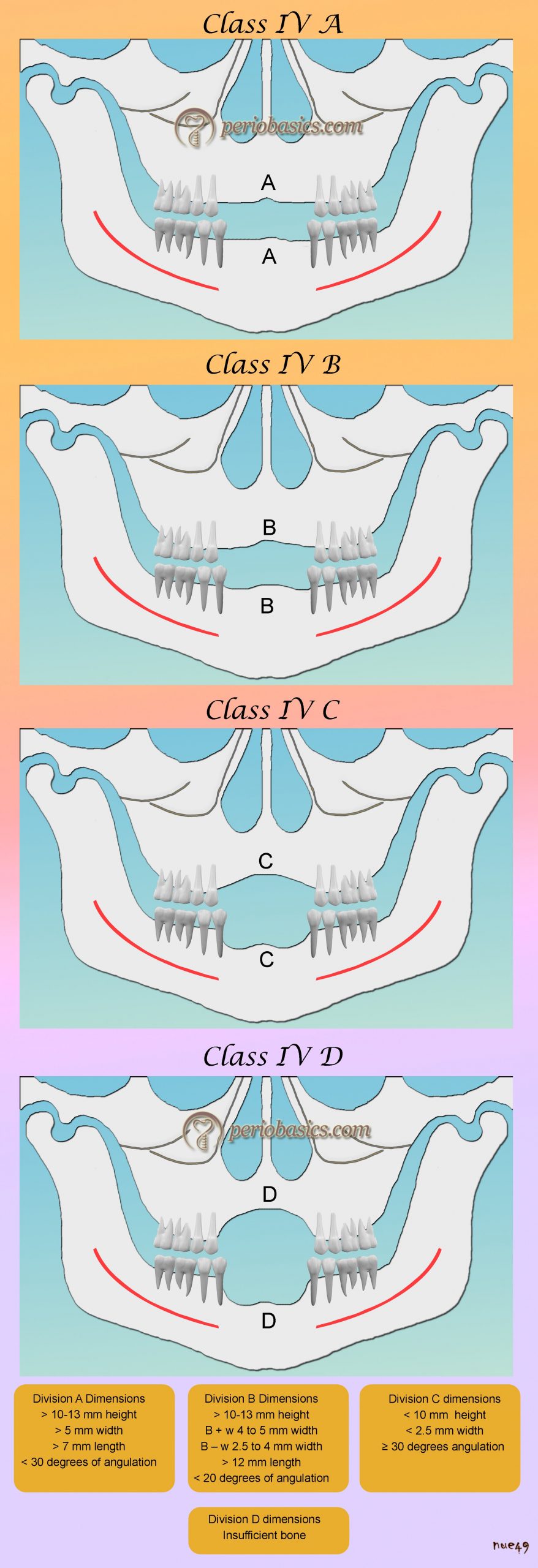
Class I: Bilateral posterior edentulous areas.
Class II: A unilateral posterior edentulous area.
Class III: Unilateral bounded partially edentulous.
Class IV: Bilateral bounded anterior partially edentulous.
Based on these four classes of partial edentulism Misch and Judy classified the available bone volume into 4 divisions A, B, C and D. They have evaluated the available bone volume in terms of the following parameters:
1. Height.
2. Width.
3. Length.
4. Angulation.
5. Crown height / Bone height (Implant body) ratio.
Let us discuss these parameters before we discuss the classification in detail.
Available Bone Height
The selection of the length of the implant fixture depends on the available bone height in an edentulous site. The available bone height is measured from the crest of the edentulous ridge to the opposing limiting anatomical landmarks such as inferior alveolar canal in the mandible and the floor of the nasal cavity and maxillary sinus in the maxilla which can be identified during radiographic assessment. Maximum bone height is available in anterior regions of the jaws. The canine eminence region in the maxilla and the first premolar region in the mandible offer the greatest bone height column of bone 9. More the height of the implant more is its surface area. An implant 3 mm longer provides more than 10% increase in surface area. The increase in length of the implant provides better initial stability, which is one of the most important factors responsible for implant success. The requirement of length is reduced in cases of dense bone where good initial stability can be achieved even with shorter implants.
In the maxillary and mandibular posterior regions due to the presence of limiting structures, i.e. maxillary sinus and mandibular canal respectively, the available bone height is less. The use of wider and shorter implants is indicated in these regions. It is recommended that 2-mm of bone height between a critical structure (inferior alveolar canal or maxillary sinus) and the implant should be maintained to avoid any surgical error.
Available Bone Width
The available bone width is measured between the facial and lingual plates at the crest of the potential implant site. Usually, the crest of the alveolar ridge is triangular in shape with a broad base. Osteoplasty in this situation provides a wide platform for the placement of implants. The problem of availability of bone width in more common with ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……….
Available Bone Length
It is the mesiodistal length of available bone in the edentulous area limited by adjacent teeth or implants. As a guideline, it is recommended that the ideal mesiodistal distance between an implant and a tooth is 1.5-2 mm and 3-4 mm between each implant. The required bone length for implant placement is actually related to the bone width. For implant diameter of 3.75 mm, the minimum bone width required is 5 mm. So, the minimum bone length required is 7 mm. In cases where the bone width available is less, the implants with smaller diameters have to be used which changes the bone length requirements also.
Available Bone Angulation
The angulation of the bone plays an important role during implant placement. The bone angulation refers to the root trajectory in relation to the occlusal plane. It is a significant feature because the occlusal forces on the implant are directed from the implant body to the surrounding bone. In mandible, the angulation of implant placement progressively increases from premolar to the second molar region because of the presence of submandibular fossa creating a deep lingual undercut. In premolar region, it is approximately 10⁰, in first molar region 15⁰ and in the second molar region around 20-25⁰. The angulation at which the maxillary central incisors can be loaded is 12⁰ 11.
Because of bone angulation, some areas in the bone do not allow us to place the implant in the desired position. The use of angled abutments in these areas helps us to achieve parallelism as well as desired positioning of the abutment.
Crown / Implant body ratio
This ratio plays an important role in the long-term success of an implant. Ideally, the crown/implant body ratio should be less than 1, i.e. the fixture should be longer than the crown portion. In cases where it is difficult to achieve, the treatment plan should be modified to incorporate more number of implants or wider implants to counter the increased stress.
Let us now, discuss the Misch and Judy classification in detail.
Misch and Judy classification for partially edentulous arches
Misch and Judy (1987) 12 classified the available bone into 4 divisions: abundant, barely sufficient, compromised, and deficient (A-D). To extend this specific organized approach to classify the bone volume, the basic four divisions have been expanded to following categories,
Division A
Division B
Division B + w (width)
Division B – w (width)
Division C
Division C – w (width)
Division C – h (height)
Division C – a (angulation)
Division D
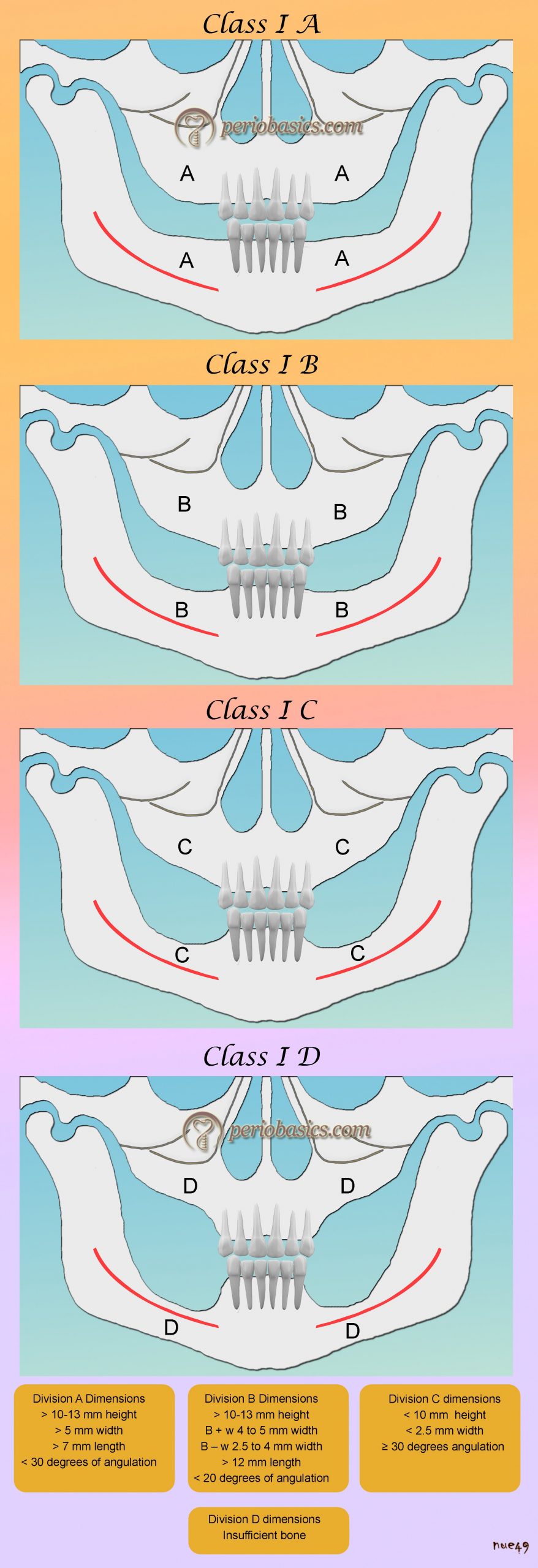


Division A (Abundant Bone)
This type of bone is available soon after tooth extraction where the bone is abundant in all the dimensions. This type of bone is usually available in anterior regions. Less bone height is available in the posterior areas of mandible and maxilla due to limiting structures. In such situations, wider implants (5 to 6 mm) may be considered in the molar regions as suitable alternatives. Due to the availability of abundant bone in all dimensions, use of root-form implants with height > 12 mm and width > 4 mm is indicated in this category. Their advantages include:
Greatest surface area.
Improved stress distribution.
Greatest range of prosthetic options.
Less fracture of implant and components.
Less abutment screw loosening.
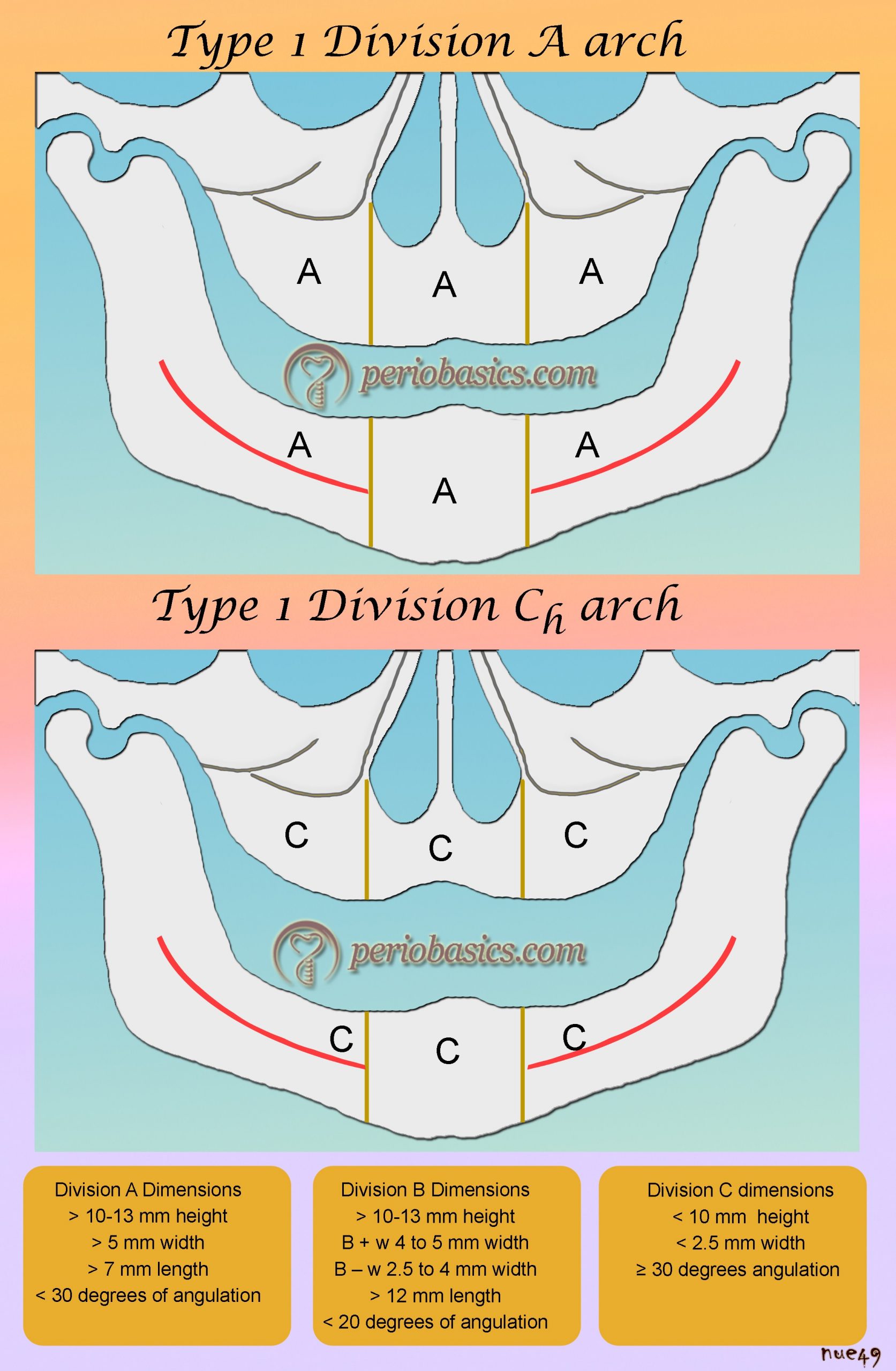
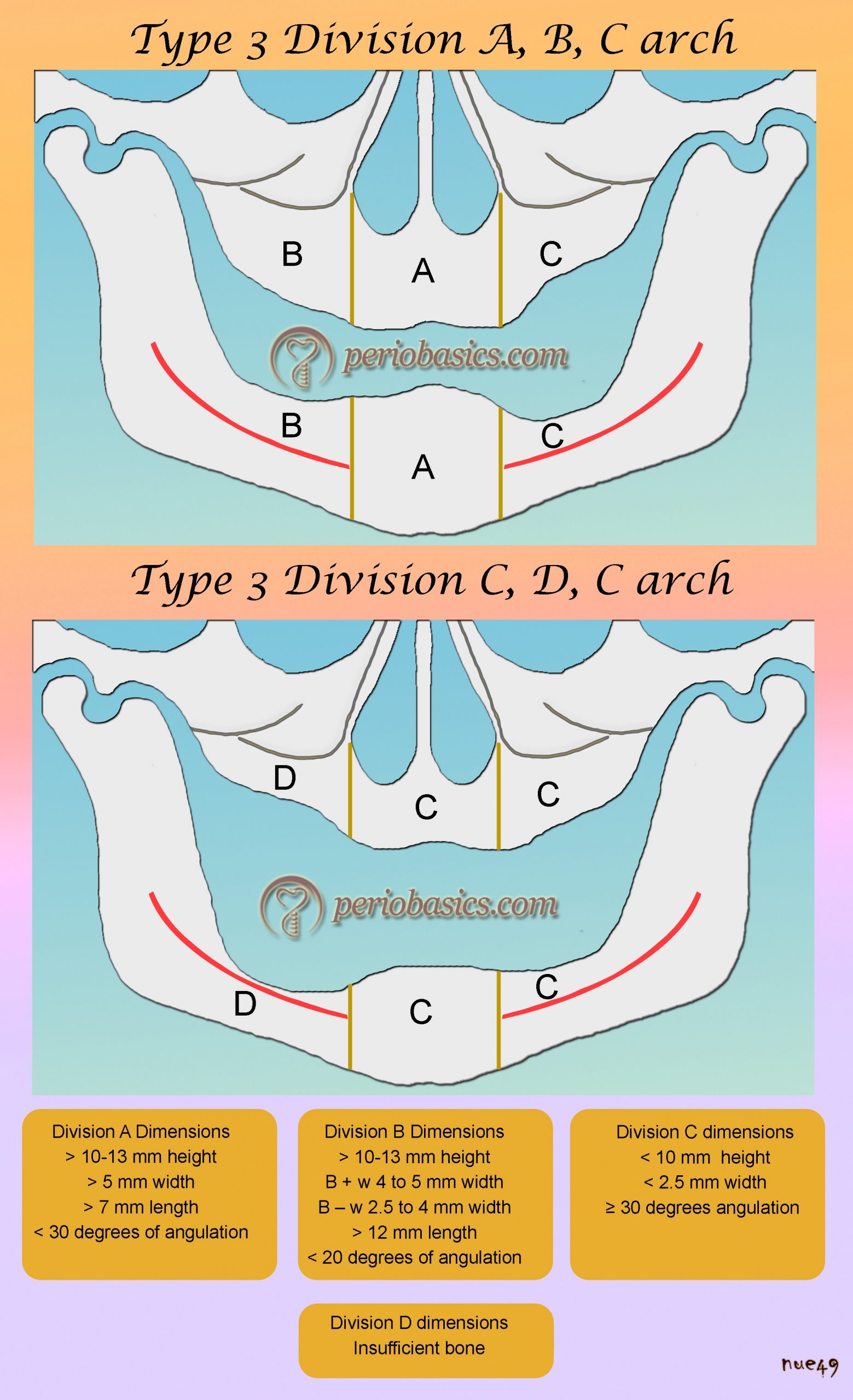
| Division A Dimensions |
|---|
| > 10-13 mm height |
| > 5 mm width |
| > 7 mm length |
| < 30 degrees of angulation |
| < 15 mm crown height |
| C/I ratio < 1 |
Treatment planning
This division of bone allows the ideal implant placement. FP-1 prosthesis (Read in detail about prosthesis in “Treatment planning for an implant patient: A general overview”) can be placed in this type of bone most of the time which gives the most esthetic results. FP-2 or FP-3 prosthesis may be considered depending on the amount of bone loss and lip positions.
If RP-4 or RP-5 prosthesis are planned, osteoplasty is required to make sufficient interarch space to accommodate the metal framework and the acrylic superstructure and overdenture attachments.
Division B (Adequate Bone)
In this type of bone, there is slight to moderate atrophy of alveolar bone. It is commonly found in posterior regions of maxilla and mandible. In this division, two subtypes (B + w and B-w) exist, depending on the extent of resorption. The available mesiodistal bone length and angulation criteria also differ as a consequence of the reduced width of the bone. Criteria of available bone height and crown height remain the same.
| Division B Dimensions |
|---|
| > 10-13 mm height |
| B + w 4 to 5 mm width |
| B – w 2.5 to 4 mm width |
| > 12 mm length |
| < 20 degrees of angulation |
| < 15 mm crown height |
| C/I ratio < 1 |
Treatment planning
The major difference between division A and B is the width of the available bone. In the case of division B, the ridge is narrower as compared to division A. In this situation osteoplasty is recommended to reduce the crest of the bone to achieve a wide platform. If by doing so, the bone height attained is greater than 12 mm, the Division B has been altered to Division A with width > 5 mm. The osteotomy done increases interarch distance which indicates the use of a FP-2 or FP-3 prosthesis to compensate for the increased interarch distance. However, the crown height/implant body ratio remains < 1 after the osteoplasty due to sufficient available bone height. If after osteoplasty the available height of bone becomes < 10 mm and C/I ratio ≥ 1, it is then considered Division C- h type of bone and treatment options will then follow those available in the Division C – h bone. Another option is to go for ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……….
Bone augmentation can be done to convert the Division B bone to Division A bone and treatment options will then follow those available for the Division A bone. The block graft either autogenous and/or demineralized freeze-dried bone (DFDB) and/or synthetic bone substitutes can be used with or without barrier membrane to increase the overall bone volume to achieve Division A bone. The augmentation requires a 4 to 6-month healing period before the placement of endosteal implants.
Division C (Compromised Bone)
Moderate to advanced atrophy is used to describe this clinical condition. The bone may be deficient in one or more dimensions. After extraction of teeth, the resorption of the bone first takes place along the width and then along the height of available bone. Keeping this thing in mind, they have given the C-w category to describe the reduced bone width. The continued resorption process causes reduced bone height, which is denoted by category C-h.
They have described one more category, C-a in which there is adequate bone both in height and width, but the angulation is greater than 30⁰. This situation is most commonly found in the anterior mandible and maxilla.
| Division C Dimensions |
|---|
| < 10 mm height |
| < 2.5 mm width |
| ≥30 degrees of angulation(Ca) |
| C/I ratio ≥1 |
Treatment planning
According to Misch 16, there are six treatment options for Division C bone which include
1. Osteoplasty
2. Root form implants.
3. Augmentation procedures.
4. Ramus frame implants.
5. Subperiosteal implants.
6. Transosteal implants.
In present scenario, out of these treatment options, augmentation procedures and root-form implants are most commonly used in the Division C-h bone. In C-h type of bone, the sub-periosteal implants can also be considered. But this is not a treatment of choice for many clinicians because of multiple problems involved.
In the case of C-w bone, osetoplasty or bone augmentation procedures are done. The augmentation procedures with block graft provide good results. A healing period of 4-6 months is required before going for implant placement.
It is better to ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Division D (Deficient Bone)
This clinical condition is used to describe the severe atrophy of bone. There is complete resorption of the alveolar bone and continued resorption of the basal bone resulting in a completely flat maxilla. The resorption of the nasal spine may also be evident. In the case of the mandible, the continued resorption up to superior genial tubercles may be evident. The completely edentulous Division D patient is the most difficult to treat because of challenging clinical procedures involved. Bone augmentation procedures have to be carried out to have sufficient support for implant placement. The surgical skill required is greater and the prosthetic outcome has a guarded prognosis. Fixed restorations are almost always contraindicated due to significant crown height. Because of the complexities involved, the complications during surgery as well as implant failures are more likely to happen in this bone division.
| Division D dimensions |
|---|
| insufficient bone |
Treatment planning
Division D (deficient bone) is most difficult to treat. In this bone type, the bone loss is severe which increases the probability of implant failure in the absence of bone augmentation to provide adequate bone support. The bone augmentation to upgrade the division of bone is highly recommended in these cases. The autogenous block graft can be done with a healing period of around 6 months before the implants are placed.
In the maxillary posterior region, sinus uplift is necessary to provide adequate bone support to implants. Care must be taken during the surgery not to perforate the Schneiderian membrane.
Subperiosteal implants are indicated in advanced ridge resorption cases, so they present a good treatment option. They are usually done in the mandible because the division D maxilla does not provide ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……….
It must be remembered that operative as well as post-operative complications are most commonly involved with treatment in Division D bone. A carefully designed treatment plan and operator’s skill are the cornerstones of the success of implant therapy in these patients.
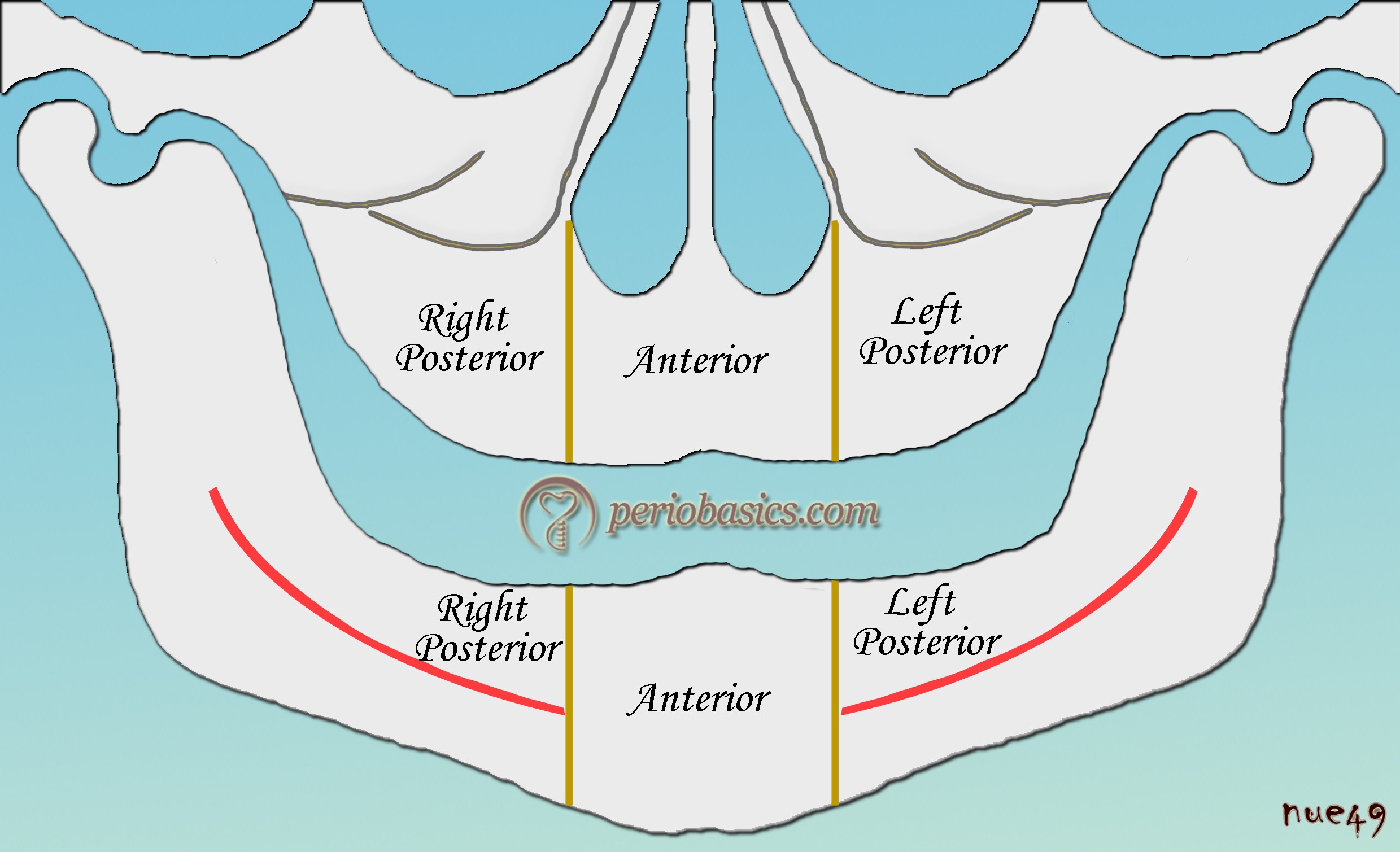
Misch and Judy classification for completely edentulous arches
Misch has classified completely edentulous arches into 3 Types. It should be noted that the classification for partially edentulous arches uses the term “Class” same as Kennedy’s classification, but classification for completely edentulous arches uses the term “Type”. The divisions of the bone volume, i.e., Division A, B, C, D are the same in both the cases. The maxilla and the mandible have been divided into three regions: the anterior region, the right region and the left region. The anterior region is the area between the first premolars in an arch. In the mandible, this area is between the mental foramen and in maxilla this area is present between the anterior limit of maxillary sinuses of both sides. The edentulous areas posterior to the anterior region are identified as right and left posterior regions accordingly.
Type 1:
In this type of edentulous arch, the bone is symmetrical and is similar in all the three segments. According to the volume of bone present, the division of the bone is written with Type 1. For example, Type 1 Division A denotes symmetrical bone in all three segments with abundant bone present. Type 1 Division C-h denotes symmetrical bone present in all three segments with an inadequate bone having a deficiency in height. Type 1 C-w indicates symmetrical bone present in all three segments with an inadequate bone with deficient bone width.
Type 2:
Here, the bone is similar in the posterior segments but differs from the anterior segment. Usually, the bone in the posterior segments is less as compared to the anterior segment. The classification of the bone is written as Type 2 + division of the bone in the anterior segment + division of the bone in the posterior segments. For example ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……….
Type 3:
In this type, the posterior segments have different bone levels. This condition is not so common, but if present should be classified as Type 3. After writing the type, the anterior bone volume division is listed first, followed by the division of the bone in the right posterior segment and then the left posterior segment. For example, Type 3 division A, B, C indicates different bone volume in the posterior quadrants with the anterior segment having Division A bone volume, the right posterior segment having B bone volume and left posterior segments having division C bone volume.

Classifications based on quality of the bone (bone density)
Linkow classification:
Linkow in 1970 17 classified bone density into the following classes,
Class I bone structure : Ideal bone type consisting of evenly spaced trabeculae and small cancellous space.
Class II bone structure: Bone with slightly large cancellous space with less uniformity of the osseous pattern.
Class III bone structure: Large marrow filled space present between the bone trabeculae.
Leckholm and Zarb classification:
Leckholm and Zarb (1985) 8 have classified the bony architecture based on the relative proportion of cortical to trabecular bone as,

Type I bone: Homogeneous cortical bone.
This type of bone has less blood supply than the rest of the types of bone. The blood supply is required for the bone to harden or calcify the bone next to the implant. Therefore, it takes approximately 5 months for this type to integrate with an implant as opposed to 4 months for Type II bone.
Type II bone: Thick cortical bone with marrow cavity.
It is considered as an ideal bone quality for implant healing. It has got an adequate blood supply and usually takes 4 months to integrate with an implant.
Type III bone: Thin cortical bone with dense trabecular bone of good strength.
Here, the bone quality is not as good as Type II bone and a 6 month time is suggested before loading an implant placed in this type of bone. Extended gradual loading of the implant can, however, improve the bone density.
Type IV bone: Very thin cortical bone with low-density trabecular bone of poor strength.
This type of bone is least favorable for implant placement. It takes the ……….Contents available in the book………..Contents available in the book………..Contents available in the book………..Contents available in the book……….
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.
India Users:
International Users:
Misch’s classification
Misch in 1988 16, classified bone into following types based on macroscopic cortical and trabecular characteristics. These are as follows,
D1 type bone
D1 type of bone is primarily composed of almost all cortical bone. A Hounsfield unit reading of 1250 and above indicates D1 bone. This type of bone is primarily present in the anterior mandible. In this type of bone, the bone to implant contact (BIC) is greatest and exceptional initial implant stability can be achieved. But, due to its high density, there are fewer blood vessels providing a significant portion of nutrient and blood supply to the periosteum.
| Clinical tip for D1 type bone |
|---|
| A conservative flap reflection is advised in this case to minimize the impact of disruption of blood vessels during and after the surgery. Another problem is the generation of heat during osteotomy. To minimize the heat production during drilling a pre-cooled sterile saline solution should be used with smaller increments in drill size with force around 2 Kg and drill speed around 2000 rpm. The drill should be used in slow pumping motion which further reduces heat generation. |
D2 type bone
In this type of bone, there is thick cortical bone, which surrounds the coarse trabecular bone. It is most suitable for implant placement and post-operative healing. This type of bone is primarily found in the anterior and posterior mandible. A Hounsfield reading between 850 to 1250 units is indicative of D2 bone.
| Clinical tip for D2 type bone |
|---|
| The bone to implant contact is significantly reduced in the D3 type of bone. A modification in the drill pattern is advised to overcome this problem. Reduced number of drills, as well as reduced drill speed (1500 rpm), are advocated in this type of bone. Care should be taken while using drills. Because of less density, there are chances of perforation of the buccal plate, especially in the maxillary anterior region. One advantage of this type of bone is high vascularity due to the fine trabecular bone. It aids in healing around the implant. Because the bone-implant contact is less, titanium plasma spray (TPS) or hydroxy-apatite (HA) coated implants are advised. |
D3 type bone
In this type of bone central fine trabecular bone is covered by a porous crestal layer of cortical bone. Commonly this type of bone is found in the anterior and posterior maxilla but also in the posterior mandible. A Hounsfield reading between 350 and 850 units is indicative of type D3 bone.
| Clinical tip for D3 type bone |
|---|
| The bone to implant contact is significantly reduced in the D3 type of bone. A modification in the drill pattern is advised to overcome this problem. Reduced number of drills, as well as reduced drill speed (1500 rpm), are advocated in this type of bone. Care should be taken while using drills. Because of less density, there are chances of perforation of the buccal plate, especially in the maxillary anterior region. One advantage of this type of bone is high vascularity due to the fine trabecular bone. It aids in healing around the implant. Because the bone-implant contact is less, titanium plasma spray (TPS) or hydroxy-apatite (HA) coated implants are advised. |
D4 type bone
This type of bone is a nightmare for implantologists. The bone is formed of fine trabecular pattern with the often absence of cortical bone. This type of bone is commonly found in the posterior maxilla. A Hounsfield reading between 150 and 350 units is indicative of D4 bone.
| Clinical tip for D4 type bone |
|---|
| In this case also a modified drill protocol is advised because the bone to implant contact is least in this case. An undersized osteotomy with use of osteotomes to condense rather than remove bone is indicated. Titanium plasma spray (TPS) or hydroxyapatite (HA) coated impl-ants may increase the predictability and success of an implant. |
D5 type bone
This is an immature and non-mineralized bone, not suitable for implant placement. A Hounsfield reading between < 150 units is indicative of D5 bone.
Conclusion
The availability of bone is the prime requirement for implant placement. The bone quantity, as well as quality, are the important determinants of the success of implant therapy. Many classifications have been proposed to classify the bone on the basis of its quality and quantity to help the clinicians to formulate a treatment plan. From the above discussion, it is clear that if the bone is deficient, the treatment plan is modified to change the design of the prosthesis or to achieve adequate bone support for the implants by performing the bone augmentation procedures. We should consider treatment options which are most suitable for a particular patient with the high prediction of success.
References
References are available in the hard-copy of the website.
Periobasics: A Textbook of Periodontics and Implantology
The book is usually delivered within one week anywhere in India and within three weeks anywhere throughout the world.